

Characterizing heterogeneity and subphenotyping acute respiratory distress syndrome with computed tomography
Garberi, R., Jabaudon, M., Bayat, S. et al. Characterizing heterogeneity and subphenotyping acute respiratory distress syndrome with computed tomography. ICMx 14, 38 (2026). https://doi.org/10.1186/s4

Summary of: Characterizing heterogeneity and subphenotyping acute respiratory distress syndrome with computed tomography — Garberi et al.
Overview
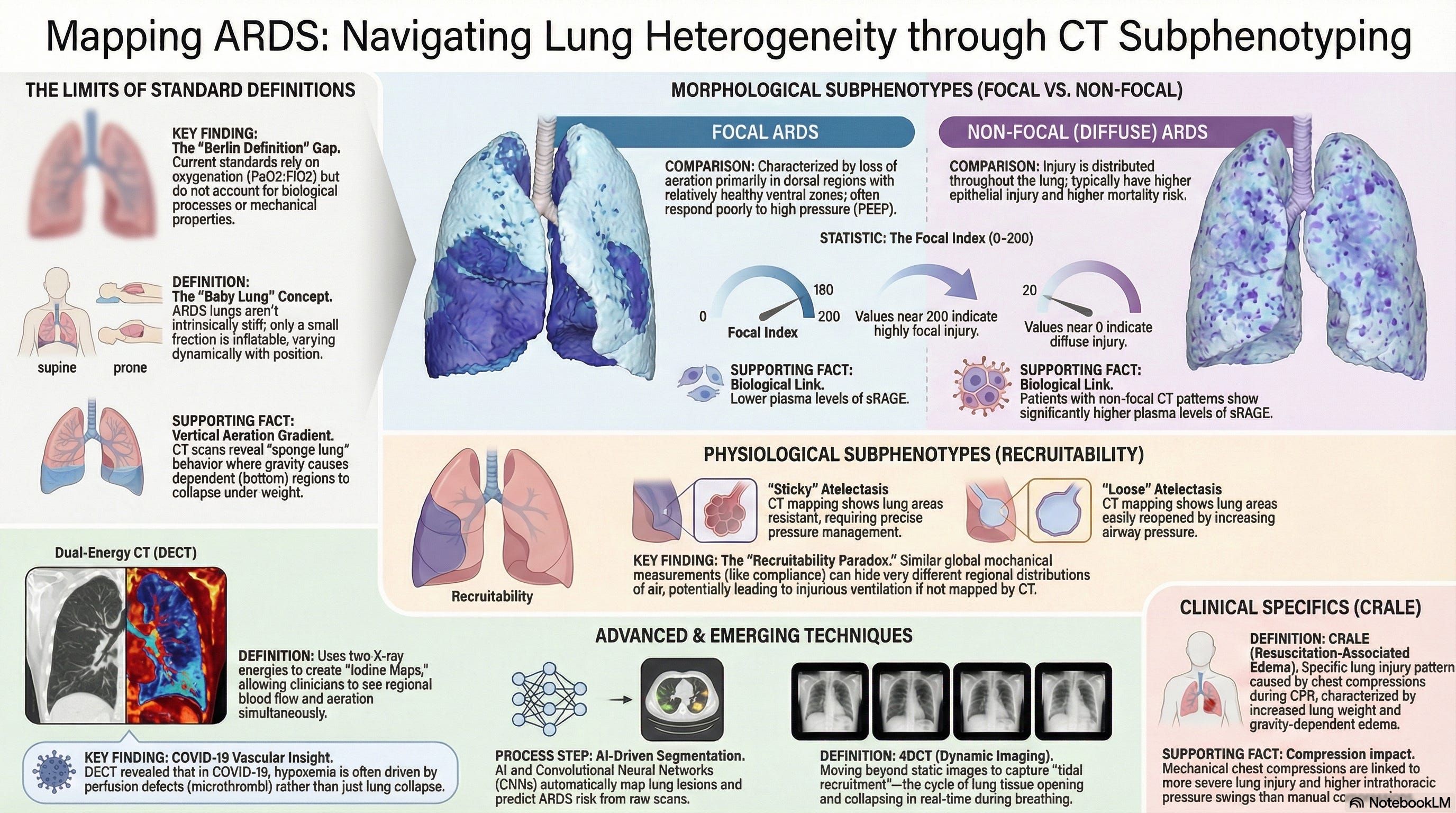
This review argues that ARDS should no longer be treated as a single radiographic or physiologic entity. Instead, CT-based phenotyping offers a more refined way to understand differences in lung morphology, recruitability, perfusion, and likely response to therapy that are not captured by oxygenation criteria alone.
Listen to the following podcast:
Key Insights
1. ARDS heterogeneity is clinically real, and oxygenation alone does not capture it.
The review emphasizes that patients meeting the same ARDS diagnostic criteria may differ substantially in lung structure, mechanics, biology, and trajectory. The Berlin framework remains useful, but hypoxemia by itself has limited prognostic discrimination and does not adequately reflect underlying morphologic heterogeneity.
2. CT adds information that bedside physiology cannot fully provide.
Computed tomography offers regional, three-dimensional assessment of aeration loss, lung density, lung weight, and perfusion abnormalities. That makes CT particularly valuable when the clinical question is not simply “how hypoxemic is the patient?” but rather “what kind of lung injury is this, where is it, and how might it respond to pressure, position, or recruitment?”
3. Morphologic patterns matter because they influence response to ventilatory strategy.
The review revisits focal versus non-focal ARDS and recruitable versus non-recruitable lungs. Focal disease tends to be more dorsal and less recruitable, with greater risk of overdistension from aggressive PEEP, whereas more diffuse patterns often show higher recruitability and may respond differently to recruitment maneuvers or higher PEEP. The paper uses this to reinforce a core principle: the same ventilator strategy may help one phenotype and harm another.
4. CT-based phenotyping is moving beyond visual description toward quantitative classification.
The review describes a progression from qualitative interpretation to semi-quantitative and quantitative CT methods, including focal indices, whole-lung recruitability estimates, and CT-derived assessments of regional opening, closing, and deformation. This shift matters because visual morphology alone can be inconsistent, while quantitative approaches may improve reproducibility and risk stratification.
5. Perfusion imaging may be one of the most important next steps.
Traditional CT is strong for morphology, but dual-energy CT expands the conversation by estimating regional perfused blood volume and helping reveal ventilation–perfusion mismatch that may not align neatly with aeration loss. This is especially relevant in conditions like COVID-19 respiratory failure, where profound hypoxemia may reflect perfusion abnormalities as much as collapse or consolidation.
6. Imaging subphenotypes are increasingly being linked to prognosis.
The review highlights work showing that CT-derived variables can improve prognostic modeling and support latent class analysis approaches that identify clinically meaningful subgroups, including recruitable versus non-recruitable classes and other imaging-informed patterns associated with different outcomes. The broader implication is that imaging may move from descriptive anatomy toward predictive enrichment.
7. The field is promising, but not yet ready for routine phenotype-guided practice everywhere.
The authors are clear that most evidence remains observational or post hoc. Advanced approaches such as deformable image registration, dynamic CT, machine learning prediction, and photon-counting CT are promising but remain largely research-facing. The main limitation is no longer whether imaging phenotypes are conceptually useful, but whether they can be measured reliably, standardized across centers, and translated into interventions that improve outcomes.
Clinical Takeaway
This review supports a practical shift in how we think about ARDS: not as one syndrome with one default ventilatory recipe, but as a collection of structural and functional phenotypes that may require different strategies. From a clinical standpoint, CT is most valuable when the team needs deeper clarification of morphology, recruitability, or perfusion burden—especially in patients whose physiology does not match the usual assumptions.
Watch the following video:
ICCN Perspective
This paper reinforces a direction that critical care has been moving toward for years:
ARDS management must become more phenotype-aware.
The major message is not that every ARDS patient needs a CT-driven protocol tomorrow. The message is that our current classification system is too shallow for true personalization. CT-based phenotyping helps explain why identical PEEP, recruitment, or positioning strategies can produce completely different results across patients. That is exactly why future ARDS care will likely depend less on broad syndrome labels and more on matching therapy to regional lung behavior.
From an ICCN standpoint, this review is valuable because it strengthens the case for precision mechanical ventilation—not in a theoretical sense, but in a structural, imaging-based, physiologic sense.
Disclaimer
Disclaimer: This content is an independent educational summary and clinical interpretation created by ICCN. It does not reproduce the original article and is not a substitute for reading the full publication. All rights to the original work belong to the respective authors and publishers. Readers are strongly encouraged to access and review the original article for complete details, methodology, and context.
Access the Original Article Here!
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
ICCN Newsletter & Educational Content Disclaimer
The content published by Interprofessional Critical Care Network (ICCN), including newsletters, articles, posts, and associated educational materials, is intended solely for educational and informational purposes. ICCN primarily references and discusses open-access scientific literature, along with publicly available research, guidelines, and expert commentary.
The views, interpretations, and opinions expressed are those of the author(s) and do not constitute medical advice, clinical recommendations, or standards of care, nor do they represent the views or policies of any employer, institution, professional society, or governing body.
All clinical content is provided to support professional education and discussion among healthcare professionals. Clinical decisions must always be made by qualified clinicians using their independent professional judgment, taking into account individual patient circumstances, institutional policies, and local regulations. ICCN does not assume responsibility or liability for any clinical decisions, actions, or outcomes resulting from the use or interpretation of the information provided.
Readers are advised to interpret all research with caution, as all scientific studies have inherent limitations, and evidence may evolve over time. ICCN makes no warranties regarding the completeness, accuracy, or applicability of the information presented.
By engaging with ICCN content, readers acknowledge and agree that ICCN, its leadership, contributors, and affiliates shall not be held liable for any claims, damages, or losses arising from the use of this material.