

Five Rights, Zero Excuses: A Framework for Ethical AI in Critical Care Research
A discipline-specific framework for investigators, peer reviewers, and editors — before undisclosed AI use damages the trust that critical care depends on.

Somewhere in an academic medical center this week, an intensivist is finishing a grant abstract with help from a chatbot. A fellow is asking a large language model to clean up the methods section of a manuscript. A peer reviewer — running late on a deadline — is pasting a confidential paper into a public AI tool to generate a review. None of this is hypothetical. All of it is happening. Almost none of it is being disclosed.
Why This Matters
Critical care does not have the luxury of waiting for AI governance to be solved somewhere else and inherited. The distance from a published ICU finding to a clinical decision at the bedside is measured in weeks, not years. A fabricated reference inside a sepsis bundle review can move through guidelines, podcasts, infographics, and institutional protocols before anyone catches the error. The Society of Critical Care Medicine has already set the principle: AI use must be reported, AI cannot be an author, humans remain accountable.¹ What the field still lacks is an actionable, ICU-specific rulebook for what that looks like across the full research lifecycle — from the moment an investigator forms a question to the moment a visual abstract drops into someone’s X feed.
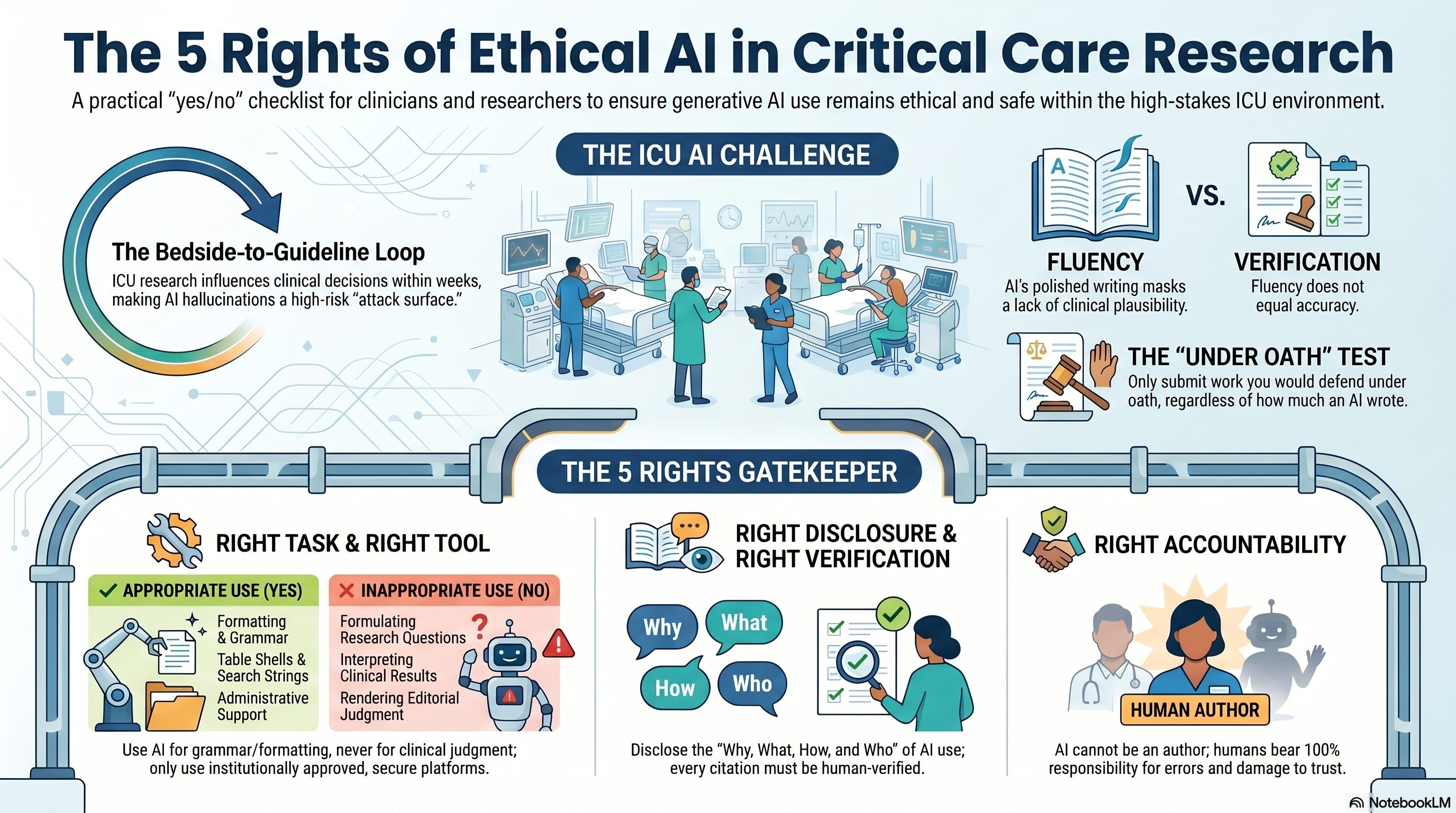
This is that rulebook. Borrowed in spirit from the nursing 5 Rights of Medication Administration — a framework every ICU clinician already carries in working memory — the five principles below are the gate every interaction with a generative AI tool should pass through before it reaches a manuscript, a peer review, or a tweetorial.
The Core Argument
Generative AI in critical care research should be treated neither as a forbidden shortcut nor as an unrestricted productivity tool. It is a high-risk cognitive assistant. Treating it that way means accepting five constraints: AI may augment, but never replace, scientific judgment; it must run on platforms that respect confidentiality; its use must be disclosed with specificity, not generalities; every output must be verified by a human expert; and accountability for what gets published rests on the human authors — fully, without escape clauses.
What the Evidence Shows
Three lines of evidence converge on the urgency of an ICU-specific framework.
First, generic publishing standards are not enough. The Committee on Publication Ethics and the World Association of Medical Editors have established that AI cannot meet authorship criteria and that its use must be disclosed.²,³ These are foundational positions, but they were written for medicine as a whole. They do not address what is distinctive about the ICU evidence pipeline: high-acuity patients, surrogate consent, messy datasets, and a downstream guideline-to-bedside loop that turns over faster than almost any other discipline in medicine.
Second, the technology’s failure modes are well documented. Systematic review evidence in npj Digital Medicine and a scoping review with ethics checklist in The Lancet Digital Health both catalog the same risk inventory: hallucinated citations, algorithmic bias, hidden training-data limitations, opacity of reasoning, and an inability to assess clinical plausibility.⁴,⁵ The 2025 consensus on implementing AI in critical care medicine reinforces that the safe path through this technology is graduated, risk-stratified, and transparent — not unrestricted.⁶
Third, the failure modes are already showing up in the literature at large. AI-generated fabricated references have triggered retractions and editorial investigations across multiple journals.⁷ No ICU-specific scandal has been documented yet, but the conditions for one — publication pressure, AI adoption, limited oversight — are already in place.
Listen to the following podcast:
Interpretation
The argument that “AI is just another tool, like a spell-checker” misreads what generative AI actually does. A spell-checker corrects a word the author already chose. A large language model generates the words, the structure, the citations, and the conclusions, and presents them with a fluency that masks how little verification has occurred. In a discipline where a misinterpreted vasopressor finding can drive shift-to-shift practice changes, fluency without verification is not a productivity gain. It is an attack surface.
The bedside test is straightforward. Would the author be comfortable defending every line of the manuscript — including the references — under oath, knowing that an AI tool wrote significant portions of it? If the answer is no, the work is not ready to ship, regardless of how polished it reads.
Bedside / Workplace Application
The five principles. Each one stands as a yes/no gate. If any answer comes back no, the investigator should not proceed.
Right Task. Grammar polishing, reference formatting, search-string generation, and table shells are appropriate uses. Formulating the research question, interpreting clinical results, drafting conclusions, and rendering editorial judgment during peer review are not. The threshold question is not whether the model can do the task — it is whether the model should, given the consequences of being wrong.
Right Tool. Consumer-facing chatbots, institutionally approved enterprise platforms, and purpose-built research tools are not interchangeable. Uploading a confidential manuscript, peer-review correspondence, or de-identified patient data to a consumer platform is a security breach regardless of the platform’s terms of service. Institutions should maintain approved tool lists. Investigators should verify approval before every use, not after.
Right Disclosure. “AI was used to assist with writing” tells editors, reviewers, and readers exactly nothing. Meaningful disclosure answers four questions: Why was AI used? What tool, including version and date? How was it used, including the actual tasks? Who verified the outputs? A structured disclosure template — operationalized like CONSORT for trials or STROBE for observational studies — makes that information auditable.
Right Verification. Every AI output that touches a research product must be independently verified by a qualified human expert. Every citation checked against the primary source. Every statistical analysis replicated with independent code. Every clinical claim traced to evidence the author has actually read. Verification is a workload — the framework does not pretend otherwise. The workload is the cost of doing this ethically.
Right Accountability. AI tools cannot be authors. They cannot hold conflicts of interest. They cannot consent to publication terms. They cannot be retracted. When something goes wrong, the human authors bear the responsibility — for the error, for the correction, and for the damage to the field’s collective trust. Accountability cannot be delegated to a disclaimer.
Teaching Pearl
The reason the nursing 5 Rights of Medication Administration is a teaching tool that works is that it is short enough to recall under cognitive load. A nurse hanging a high-alert medication at 3 a.m. does not need a 40-page policy document — they need five questions they can run through in fifteen seconds. The same logic applies to AI in research. The 5 Rights are not a substitute for institutional governance, IRB review, or journal policy. They are the working-memory checklist a clinician-investigator can run before clicking submit. Embed them at the front of fellowship curricula, RT research training, and nursing-led QI work, and the framework becomes culture instead of policy.
Counterpoints and Caveats
The strongest objection to a discipline-specific framework is that AI will outrun it. Multimodal systems, autonomous research agents, and AI-human collaborative platforms will change what “AI use” even means within the next year. The 5 Rights are deliberately framed as principles rather than tool-specific rules so they survive that turnover — but they will need updating as the technology matures. A second objection is that some investigators, especially those in low-resource settings, may not have access to the enterprise-grade tools the framework presumes. That is a real equity concern. The fix is institutional and societal — SCCM, journals, and academic medical centers can negotiate enterprise access for the global critical care community — not relaxation of the rule.
Limitations of the Argument
This framework is a starting point, not a finished product. It has not been empirically tested for whether it changes investigator behavior, and its effectiveness as a teaching tool remains to be measured. Its center of gravity is the SCCM journal family and North American institutional practice; non-U.S. critical care communities may face different regulatory environments and resource constraints that require adaptation. And the framework presumes a research culture in which the author team takes verification seriously enough to do it. In a culture that does not, no checklist will prevent misuse — which is why the framework needs institutional reinforcement, not just publication.
Bottom Line
Generative AI is already inside the critical care research enterprise. The choice is no longer whether to permit it. The choice is whether to govern it explicitly, with a discipline-specific framework the field actually applies, or to let undisclosed use compound until the first scandal forces a reactive fix. The 5 Rights are an attempt at the former. If the answer to any of the five questions is no, the investigator should not proceed.
References
Buchman TG, Tasker RC. Fair use of augmented intelligence and artificial intelligence in the preparation and review of submissions to the Society of Critical Care Medicine journals: Critical Care Medicine, Pediatric Critical Care Medicine, and Critical Care Explorations. Crit Care Med. 2024;52:e100-e106. doi:10.1097/CCM.0000000000006066
Committee on Publication Ethics. Authorship and AI tools. COPE Position Statement. Available at: https://publicationethics.org/guidance/cope-position/authorship-and-ai-tools. Accessed April 28, 2026.
Zielinski C, Winker MA, Aggarwal R, et al. Chatbots, generative AI, and scholarly manuscripts: WAME recommendations on chatbots and generative artificial intelligence in relation to scholarly publications. Res Integr Peer Rev. 2023;8:10.
Haltaufderheide J, Ranisch R. The ethics of ChatGPT in medicine and healthcare: A systematic review on large language models (LLMs). NPJ Digit Med. 2024;7:183.
Ning Y, Teixayavong S, Shang Y, et al. Generative artificial intelligence and ethical considerations in health care: A scoping review and ethics checklist. Lancet Digit Health. 2024;6:e848-e856.
Cecconi M, De Backer D, Antonelli M, et al. Implementing artificial intelligence in critical care medicine: A consensus of 22. Crit Care. 2025;29:290.
Stokel-Walker C, Van Noorden R. What ChatGPT and generative AI mean for science. Nature. 2023;614:214-216.
Mollaki V. Death of a reviewer or death of peer review integrity? The challenges of using AI tools in peer reviewing and the need to go beyond publishing policies. Account Res. 2024;31:478-495.
Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: Updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024;385:e078378.
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.
🌐 ICCN Has a New Home: iccn.io
The Interprofessional Critical Care Network just launched its new website — iccn.io — built to be the single hub for everything ICCN: clinical intelligence, the daily Substack, educational resources, and the interprofessional community connecting RTs, intensivists, nurses, PAs, NPs, and pharmacists around better critical care.
If this framework is the kind of synthesis you want more of, iccn.io is where it lives. Bookmark it, explore it, and join the network shaping the future of the ICU.