

Lung Protection Ends Where Drive Begins
The 2026 Case for Treating Respiratory Effort as a Vital Sign in the ICU

Every Tuesday at ICCN I come back to the same uncomfortable question. We measure tidal volume, plateau pressure, driving pressure, mechanical power, PEEP, and FiO₂, and we have built a lung-protective number set that earned its place in the ARDS Network era. A growing body of work, capped by a 2026 Current Opinion in Critical Care review, says the most dangerous variable in the room is the one we still cannot read off the ventilator. It is the patient’s own effort.
Why This Matters
P-SILI, patient self-inflicted lung injury, is the proposition that a patient with injured lungs can wound themselves further with the breath they generate. Brochard, Slutsky, and Pesenti put the term into formal print in 2017, arguing that uncontrolled inspiratory effort produces transpulmonary pressures and regional strains that mirror, and at times exceed, what an aggressive ventilator can deliver.² The premise has been contested loudly and productively. It is no longer a fringe idea in 2026. The new Current Opinion review by Balzani, Alcala, Bellani, and Pesenti maps a decade of mechanistic, observational, and trial-adjacent data and reaches a conclusion that should rearrange how every ICU thinks about respiratory failure. High drive and high effort track with disease severity, and the accumulating physiology supports a causal contribution to lung injury, diaphragm injury, and mortality in patients who are spontaneously breathing, on noninvasive support, or in assisted modes on the ventilator.¹
The implication for the interprofessional ICU team is direct. If effort can hurt the lungs, then drive is a vital sign, and a vital sign needs numbers, alarms, and a plan. Respiratory therapists who own the ventilator, intensivists who own the trajectory, nurses who own the bedside detection, pharmacists who own the sedation strategy, APPs who own the daily plan, and perfusionists who manage extracorporeal escape routes are all part of a system that, today, mostly flies blind on this variable.
Built for You. Live Now.
The new ICCN website is open. Two features are worth a look. The Research section organizes our coverage of the trials and reviews driving practice change, by system and continuously updated from 26 different journals. The Article section holds the full ICCN back catalog, searchable and free to browse. Both are built to the same standard as the Substack you are reading. Explore ICCN.
The Study / Evidence in Context
The anchor for this article is the February 2026 Current Opinion in Critical Care narrative review of P-SILI by Balzani, Alcala, Bellani, and Pesenti.¹ It is a structured synthesis of mechanistic experiments, recent clinical data, and pharmacologic and ventilatory interventions intended to limit injurious effort while preserving diaphragmatic function. It sits at the same editorial intersection as Tonelli and colleagues’ 2025 Critical Care consensus on bedside drive and effort assessment, a 28-author document signed by most of the names that have built this field over the last fifteen years.⁶
The historical scaffolding under that synthesis is worth restating, because fellows and new RTs often inherit the answer without inheriting the argument. The seminal experimental work belongs to Yoshida and colleagues. In a 2012 paper they showed that strong spontaneous effort in a severely injured lung model produced transpulmonary pressures and regional strains that worsened injury, even when the ventilator was set to deliver a textbook low tidal volume.⁵ A year later, the same group used electrical impedance tomography to expose a phenomenon they called occult pendelluft. Gas oscillates from non-dependent to dependent lung regions during early inspiration, redistributing strain into the most vulnerable territory without changing what the ventilator screen reports as tidal volume.³ Brochard, Slutsky, and Pesenti gathered that experimental thread, added the clinical pattern recognition coming out of acute hypoxemic respiratory failure cohorts, and named the syndrome P-SILI.²
The Balzani synthesis updates this story with mechanistic granularity. The injurious pathway runs through four overlapping channels. Global and regional overdistension from vigorous effort. Increased pulmonary perfusion and negative-pressure pulmonary edema during deep pleural pressure swings. Pendelluft-driven local strain. And patient-ventilator asynchrony that compounds all three.¹ The authors highlight large prognostic datasets showing that elevated airway occlusion pressure (P0.1), esophageal pressure swings, and the pressure-muscle index correlate with worse ICU survival and prolonged ventilation, even after adjustment for disease severity.¹
The clinical translation has been moving in parallel. Tonelli and colleagues showed in 2020 that the magnitude of esophageal pressure swing within two hours of starting noninvasive ventilation predicted intubation in de novo hypoxemic respiratory failure. Patients who lost their effort burden early did well. Patients who held high effort despite NIV failed.⁷ Marongiu and colleagues, in their 2024 J Clin Med review, organized the bedside evidence and emphasized that early drive assessment identifies the patients at highest risk of injury before the chest film tells you that something has gone wrong.⁸ Grieco and colleagues, in the 2021 HENIVOT trial, reported that helmet noninvasive ventilation reduced the rate of intubation and invasive ventilation days in COVID-19 patients with moderate to severe hypoxemic respiratory failure compared with high-flow nasal oxygen, a finding most readily explained by the lower pleural pressure swings and reduced effort that helmet NIV imposes.¹³
The neuromuscular blockade era informs the same story from the other side. The 2010 ACURASYS trial of cisatracurium in early severe ARDS showed a survival signal that was widely interpreted as the benefit of taking effort off the table.⁹ The 2019 ROSE trial, performed against a backdrop of higher PEEP and lighter sedation in the control arm, did not reproduce that survival benefit and changed practice toward selective rather than routine paralysis.¹⁰ Both trials remain in scope for the P-SILI conversation. The divergence is most coherently explained by the fact that the ROSE control arm already protected against high-effort injury through PEEP titration and lighter sedation targets that allowed mobilization without permitting vigorous effort, while ACURASYS used a deeper sedation comparator with less protection from drive in the control group.
What Stood Out
A few findings from the Balzani review and adjacent literature should reorganize how the interprofessional team reads the ventilator and the patient on top of it.
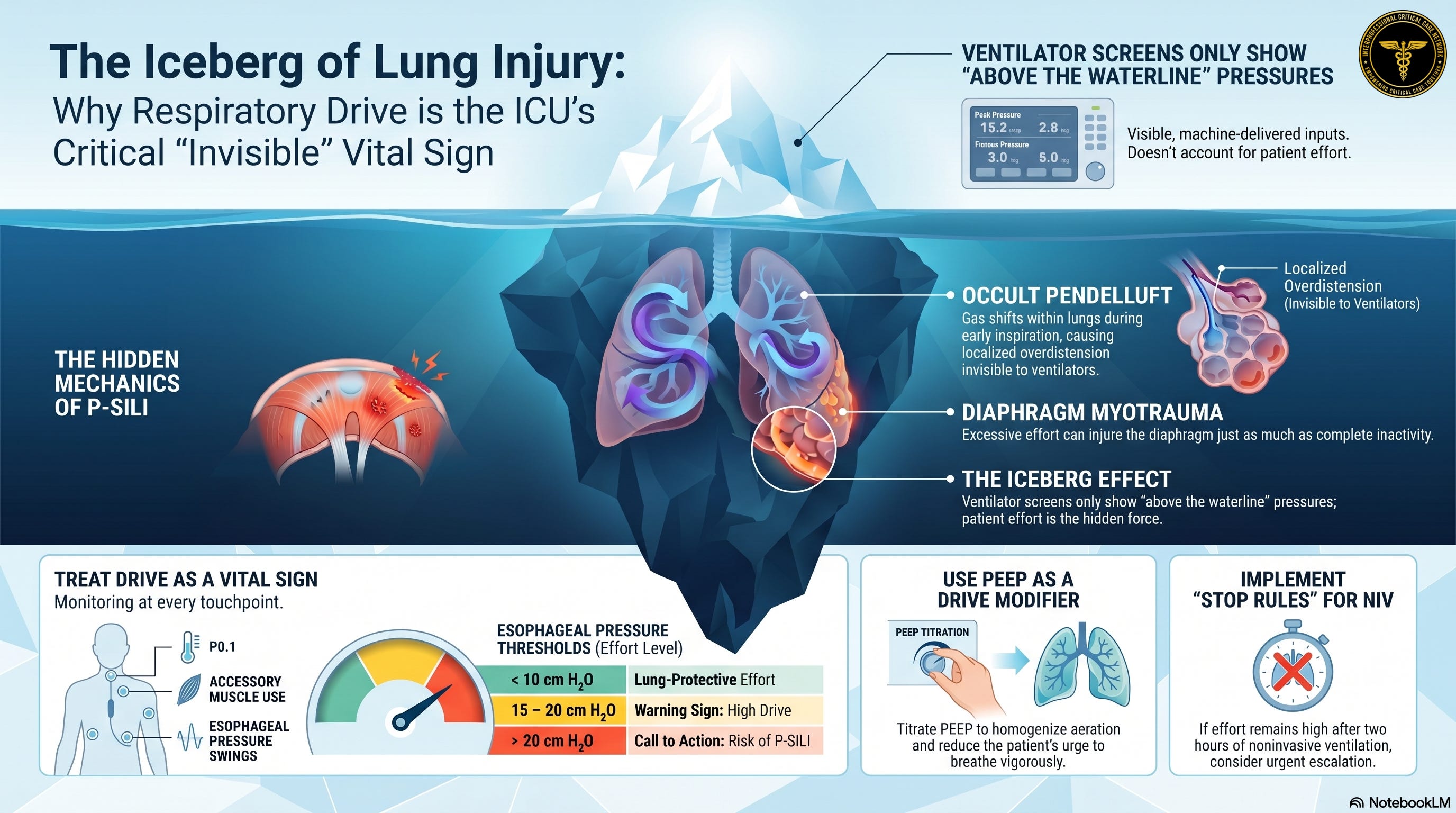
First, the iceberg argument. Total lung stress during spontaneous or assisted breathing is the sum of the pressure the ventilator delivers and the pressure the patient generates with the diaphragm and accessory muscles. The ventilator shows what is above the waterline. The pleural pressure swing, the part that comes from the patient, is the iceberg below. A 6 mL/kg tidal volume that looks protective on the screen can be associated with regional strains in the dependent lung that match or exceed a 12 mL/kg breath in a passively ventilated patient.¹ ⁵ This is the central mechanism by which a textbook ventilator setting can fail an actively breathing patient.
Second, pendelluft is not a curiosity. Yoshida’s 2013 electrical impedance tomography study and the confirmatory work that followed demonstrated that gas can move from the non-dependent lung to the dependent lung in early inspiration without changing measured tidal volume. The dependent lung receives a regional volume that exceeds what the ventilator believes it delivered, producing focal overdistension, cyclic recruitment, and inflammatory amplification in exactly the territory that is already inflamed.³ ⁴ Patient-ventilator asynchrony amplifies this in proportion to drive.
Third, the cardiovascular cost is not abstract. Strong inspiratory effort generates negative intrathoracic pressure, which increases venous return, increases pulmonary capillary transmural pressure, and shifts fluid into the interstitium. In a permeability-injured lung, this directly worsens edema. Right ventricular afterload climbs at the same moment, while left ventricular filling is impaired by ventricular interdependence. These effects compound on the lungs, the heart, and the gas exchange surface in series.¹
Fourth, the diaphragm is part of the injury. Goligher and colleagues, in their 2015 ultrasound cohort and the 2020 perspective on lung- and diaphragm-protective ventilation, showed that diaphragm thickness changes within the first week of mechanical ventilation in most critically ill patients. Loss of thickness greater than 10 percent is associated with prolonged ventilation. An increase greater than 10 percent, the pattern produced by excessive effort, is associated with worse outcomes through a different mechanism known as under-assistance myotrauma.¹¹ ¹² A diaphragm thickening fraction in the 15 to 30 percent range, the value of a healthy adult at rest, correlated with the shortest duration of mechanical ventilation.¹¹ The implication is uncomfortable. The same patient who is hurting their lungs with high drive may be injuring their diaphragm in the same breath.
Fifth, drive and effort can be measured at the bedside. The Tonelli 2025 consensus catalogs the available techniques. Esophageal manometry as the gold standard for inspiratory effort. Electrical activity of the diaphragm via the Edi catheter. The airway occlusion pressure P0.1. The inspiratory pressure during an end-expiratory hold (Pocc). Expiratory hold maneuvers. Diaphragm ultrasound thickening fraction. And an expanding set of ventilator-derived surrogates including the flow index.⁶ Not every ICU has every tool. Every ICU has some.
Watch the following video:
The most dangerous tidal volume in modern critical care is the one the ventilator does not show you.
Physiologic, Clinical, Leadership, or Ethical Interpretation
Here is my read.
For fifteen years we have treated mechanical ventilation as a problem of what the machine does to the lung. The 6 mL/kg tidal volume revolution, the driving pressure threshold of 14 to 15 cm H₂O, the mechanical power conversation, the prone position trials, and the PEEP titration literature are all built on a single architectural premise. Control the inputs from the ventilator and you control lung-side stress and strain. That premise is incomplete.
In an awake or assisted patient with injured lungs, the dominant source of stress and strain may be the patient. Ventilator dials do not reach that source directly. They can only modulate it, sometimes for the better, sometimes for the worse. PEEP titrated up may homogenize ventilation, reduce strain rate, and convert a high-drive breath into a tolerable one. PEEP titrated down may have the opposite effect. Pressure support increased to lower the work of breathing may suppress drive in some patients and intensify it in others. There is no single setting that universally fixes the problem, because the problem is in the brainstem and the chemoreceptors.
This reframes the daily ICU plan for every discipline at the bedside.
The respiratory therapist’s role expands. Vent settings are still the deliverable. But the diagnostic question changes. What is this patient’s drive, and how does this setting change it. RTs who carry the esophageal balloon, the ultrasound probe, the EIT belt where available, and the experience to read a flow-time waveform asynchrony pattern own the toolset that makes drive visible to the rest of the team.
The intensivist’s role changes from prescriber to integrator. The question is no longer only what mode and what targets. It is what physiologic phenotype is this patient occupying right now, and what is the minimum-injury combination of ventilation, sedation, position, and adjunct that we can build for the next eight hours. The integrator role implies more frequent and more granular communication with the bedside RT and nurse, not less.
The nurse’s role becomes the early warning system. Tachypnea above thirty, accessory muscle recruitment, paradoxical abdominal motion, suprasternal indrawing, and the patient’s own report of dyspnea are the most accessible drive surrogates we have. They are at the bedside continuously in a way no other team member is. A drive-aware nurse identifies the patient who needs an urgent ventilator and effort assessment before the chest film, the gas, or the imaging catches up.
The pharmacist’s role evolves. Sedation as a drive-modifying intervention deserves a separate conversation in every drive-elevated patient. Propofol and dexmedetomidine modulate drive differently. Opioids reduce drive at a cost. Neuromuscular blockade abolishes effort entirely at a different cost. The pharmacist who reads the drive plan and tailors the sedation strategy to it is doing P-SILI prevention work, even if no one in the room uses the term.
The APP’s role is to carry the plan across shifts. Drive-aware care is sustained only if it is documented and signed out. The APP who closes the loop between the morning intensivist plan and the evening RT bedside reality is the person who keeps a drive-targeted strategy from drifting back to a tidal-volume-only protocol within twelve hours.
The perfusionist’s role enters when the lung cannot be protected by any combination of the above. Venovenous extracorporeal CO₂ removal and full VV ECMO support exist precisely to convert a patient who cannot be made safe on the ventilator into one who can be paralyzed or rested on lung-rest settings until the underlying injury resolves. The Balzani review names extracorporeal CO₂ removal explicitly as part of the modern P-SILI toolkit.¹
This is interprofessional medicine in its sharpest form. No single discipline can solve P-SILI alone. Every discipline holds a tool the others cannot use.
Listen to the following podcast:
Bedside / Workplace Takeaways
Treat drive as a vital sign. When a patient is on noninvasive ventilation, high-flow nasal oxygen, or any assisted mode of invasive ventilation, build a habit of explicitly assessing drive and effort at every team touchpoint. Respiratory rate, accessory muscle use, dyspnea report, tidal volume in pressure-targeted modes, and esophageal pressure swing where available. If you cannot answer the question “what is this patient’s drive,” you do not yet have a complete plan.
Read pleural pressure when you can. Esophageal manometry remains the bedside reference standard for inspiratory effort.⁶ ⁷ A delta esophageal pressure swing under 10 cm H₂O is generally compatible with lung-protective effort. A swing consistently above 15 cm H₂O in an injured lung is a warning sign. Above 20 cm H₂O is a call to action.
Use PEEP as a drive-modifying lever, not only a recruitment lever. Adequate PEEP can convert an injurious spontaneous breath into a safer one by homogenizing aeration and reducing pendelluft.¹ ⁵ When you escalate PEEP in an assisted breather, ask not only “did oxygenation improve,” but “did effort decrease.”
Have a stop rule for noninvasive support. Tonelli’s 2020 work made the case that early failure to reduce effort on NIV predicts intubation.⁷ A patient who is two hours into NIV with persistent high effort, persistent tachypnea above thirty, persistent accessory muscle use, and rising drive markers is at risk of P-SILI on top of their original disease. Delayed intubation in that population is not a kindness.
Match sedation strategy to drive phenotype. Light sedation is the default in the post-ROSE era, and that is the right default. The exception is the patient whose drive remains injurious despite optimal ventilator and PEEP settings. In that patient, deepening sedation, adding an opioid, or proceeding to neuromuscular blockade is a lung-protective act, not a regression to old practice.⁹ ¹⁰
Protect the diaphragm in parallel with the lung. A diaphragm thickening fraction of 15 to 30 percent is the target.¹¹ Under-assistance and over-assistance both injure. If your RT and nurse are titrating pressure support to that range with ultrasound feedback, you are doing modern care. If you are setting pressure support to a number once a day and revisiting at rounds, you are not.
Escalate to extracorporeal support when the lung cannot be protected at the bedside. Patients with refractory high drive, refractory hypoxemia, or refractory hypercapnia despite optimal ventilator, prone positioning, sedation, and paralysis are candidates for VV-ECMO or extracorporeal CO₂ removal evaluation.¹ Earlier consultation with the ECMO and perfusion team is part of the P-SILI strategy.
Teaching Pearl
The next time you stand at the bedside of a tachypneic patient in respiratory failure, ask yourself a single question before you touch the ventilator. Where is most of the work of this breath coming from. If the answer is the patient, you have a P-SILI problem on your hands, and the solution lives in some combination of PEEP, mode, sedation, paralysis, position, and (when those run out) extracorporeal support. The tidal volume on the screen is the last number you should be looking at.
Teach your fellows, your new respiratory therapists, your nurses, and your APPs the iceberg image. The visible part is what the ventilator shows. The hidden part is what the patient generates. The patient who is hurting their lungs with their own breath looks fine on a screen until the moment they do not.
What We Should Not Over-Assume
P-SILI as a concept remains contested in important ways and the 2026 evidence does not close that conversation. The causal claim, that high drive injures the lung rather than reflecting a sicker lung, is supported by mechanistic and observational work, and by trials of effort removal, but no large multicenter trial has tested a drive-targeted strategy against a non-drive-targeted strategy with mortality as the primary outcome.¹ ¹⁵ Tobin and colleagues have argued forcefully that the data so far cannot exclude reverse causation. Patients with worse lungs simply have higher drive, and intervening on drive does not necessarily change the trajectory.¹⁵ That is a legitimate counterposition and it deserves a place in every teaching conference.
The clinical corollary is that we should not adopt an aggressive intubate-to-prevent-P-SILI doctrine in the absence of trial evidence. Patel and colleagues pointed out in 2017 that intubation, deep sedation, and paralysis carry their own injury portfolio. Delayed extubation, ICU-acquired weakness, and post-ICU cognitive impairment all sit on the cost side of that ledger.¹⁴ Drive-aware care is different from early-intubation doctrine. The drive-aware ICU watches drive, optimizes the modifiable variables, and reserves intubation for the patient in whom the modifiable variables have run out.
Limitations
The Balzani review is a narrative synthesis rather than a systematic one, which is the appropriate format for a field that does not yet have the multicenter randomized trials it needs.¹ The bedside drive assessment literature, much of which is summarized in the 2025 Tonelli consensus, has not yet produced a single validated cutoff that should trigger a specific action across all ICUs and all phenotypes.⁶ The translational gap from physiology to mortality endpoint remains. Most of the available signal is at the level of intermediate outcomes such as oxygenation, mechanical work, biomarkers, and intubation rates. The field needs a drive-targeted trial in 2027 or 2028 that pits a structured effort-monitoring strategy against contemporary care with mortality as the primary outcome. Until that trial exists, the evidence we have should inform pattern recognition and bedside escalation rather than rigid protocol.
Bottom Line
The 2026 evidence makes the case I have been waiting to make for years on the Tuesday slot at ICCN. Lung protection is incomplete without effort protection. If we are not measuring drive at the bedside, we are not protecting the lung in the awake or assisted patient. The next era of mechanical ventilation belongs to the interprofessional teams that build a drive-aware workflow now, before the trial that mandates it arrives.
Javier Amador-Castaneda, BHS, RRT, FCCM | Founder & CEO, ICCN
Reference
Balzani E, Alcala GC, Bellani G, Pesenti A. Patient self-inflicted lung injury an important phenomenon. Curr Opin Crit Care. 2026;32(1):9-16. doi:10.1097/MCC.0000000000001348
Brochard L, Slutsky A, Pesenti A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am J Respir Crit Care Med. 2017;195(4):438-442. doi:10.1164/rccm.201605-1081CP
Yoshida T, Torsani V, Gomes S, et al. Spontaneous effort causes occult pendelluft during mechanical ventilation. Am J Respir Crit Care Med. 2013;188(12):1420-1427. doi:10.1164/rccm.201303-0539OC
Yoshida T, Fujino Y, Amato MB, Kavanagh BP. Fifty years of research in ARDS. Spontaneous breathing during mechanical ventilation. Risks, mechanisms, and management. Am J Respir Crit Care Med. 2017;195(8):985-992. doi:10.1164/rccm.201604-0748CP
Yoshida T, Uchiyama A, Matsuura N, Mashimo T, Fujino Y. Spontaneous breathing during lung-protective ventilation in an experimental acute lung injury model: high transpulmonary pressure associated with strong spontaneous breathing effort may worsen lung injury. Crit Care Med. 2012;40(5):1578-1585.
Tonelli R, Protti A, Spinelli E, et al. Assessing inspiratory drive and effort in critically ill patients at the bedside. Crit Care. 2025;29(1):339. doi:10.1186/s13054-025-05526-0
Tonelli R, Fantini R, Tabbì L, et al. Early inspiratory effort assessment by esophageal manometry predicts noninvasive ventilation outcome in de novo respiratory failure: a pilot study. Am J Respir Crit Care Med. 2020;202(4):558-567. doi:10.1164/rccm.201912-2512OC
Marongiu I, Slobod D, Leali M, Spinelli E, Mauri T. Clinical and experimental evidence for patient self-inflicted lung injury (P-SILI) and bedside monitoring. J Clin Med. 2024;13(14):4018. doi:10.3390/jcm13144018
Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107-1116. doi:10.1056/NEJMoa1005372
National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss M, Huang DT, Brower RG, et al. Early neuromuscular blockade in the acute respiratory distress syndrome. N Engl J Med. 2019;380(21):1997-2008. doi:10.1056/NEJMoa1901686
Goligher EC, Fan E, Herridge MS, et al. Evolution of diaphragm thickness during mechanical ventilation. Impact of inspiratory effort. Am J Respir Crit Care Med. 2015;192(9):1080-1088. doi:10.1164/rccm.201503-0620OC
Goligher EC, Dres M, Patel BK, et al. Lung- and diaphragm-protective ventilation. Am J Respir Crit Care Med. 2020;202(7):950-961. doi:10.1164/rccm.202003-0655CP
Grieco DL, Menga LS, Cesarano M, et al. Effect of helmet noninvasive ventilation vs high-flow nasal oxygen on days free of respiratory support in patients with COVID-19 and moderate to severe hypoxemic respiratory failure: the HENIVOT randomized clinical trial. JAMA. 2021;325(17):1731-1743. doi:10.1001/jama.2021.4682
Patel BK, Wolfe KS, Hall JB, Kress JP. A word of caution regarding patient self-inflicted lung injury and prophylactic intubation. Am J Respir Crit Care Med. 2017;196(7):936. doi:10.1164/rccm.201702-0410LE
Tobin MJ, Laghi F, Jubran A. P-SILI is not justification for intubation of COVID-19 patients. Ann Intensive Care. 2020;10(1):105. doi:10.1186/s13613-020-00724-1
Clinical Disclaimer
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.