

Refractory Septic Shock Finally Has a Definition, and It Will Change How You Triage the Sickest Patient on Your Unit
Fifty-six experts. Twenty-two countries. Five Delphi rounds. Thirteen criteria. The phrase the bedside has been using for thirty years just got operational rules.

For the better part of three decades, “refractory septic shock” has been doing heavy lifting at the bedside, in journal clubs, in trial inclusion criteria, and in the conversations clinicians have with families when the catecholamines stop working. The phrase carried clinical weight. It did not carry a definition.
That changed on March 24, 2026, when the Society of Critical Care Medicine and the European Society of Intensive Care Medicine jointly published the first international consensus criteria for refractory septic shock in Intensive Care Medicine and Critical Care Medicine. Co-chaired by Marc Leone and Ashish Khanna, the work is the product of a five-round Delphi process across 56 panellists from 22 countries on five continents. It gives the most severe form of septic shock something it has never had: a shared, operational, bedside-deployable diagnostic framework.
The implication for the Monday morning ICU is not subtle. The patient you have been calling refractory based on a gestalt of high norepinephrine plus a stubborn lactate now belongs to a phenotype with criteria. That phenotype will drive enrollment in next-generation rescue-therapy trials. It will shape how SSC 2026 is read. It will change the language interprofessional teams use when escalating care.
Why This Matters
Every ICU clinician sees this patient: physician, RT, nurse, advanced practice provider, pharmacist, perfusionist. Multiple times a week. The septic shock case that started on the standard hour-1 bundle, has cleared two liters of balanced crystalloid, is on norepinephrine that keeps climbing, has a lactate that will not budge below 4 mmol/L, and is producing a mottled knee, a delayed capillary refill, and a phone call from the bedside RN that begins with “We’re not getting anywhere.”
That patient has always existed. What has never existed was a shared language for that patient. A 2023 systematic review identified at least a dozen overlapping and inconsistent definitions of refractory septic shock in the published literature, with norepinephrine thresholds ranging from 0.1 to 1.0 µg/kg/min, lactate cutoffs spanning 2 to 4 mmol/L, and inclusion criteria that often contradicted each other across studies on the same therapeutic question.
The cost of that ambiguity is real. It blocks meta-analysis of rescue therapies such as angiotensin II, hydrocortisone, hemoadsorption, and methylene blue, because the populations under study are not the same population. It muddies prognostic conversations with families. It makes interprofessional handoffs sloppier than they should be when the words mean different things to the receiving team. It leaves the sickest cohort of septic patients without a standardized framework for escalation.
The new SCCM/ESICM consensus does not solve every disagreement. It stakes ground that the field can build on. It does so at a moment when sepsis resuscitation is moving faster than it has in a decade, with SSC 2026 just released, ANDROMEDA-SHOCK-2 just published, and ESICM circulatory shock guidelines just updated.
The Study / Evidence in Context
The methodology underneath the consensus matters because Delphi work is only as defensible as the panel that produces it. The steering committee included Leone, Khanna, Myatra, Dugar, Russell, and Wieruszewski, drawing from two societies that together represent the dominant global voice in adult critical care. The panel itself was assembled with explicit attention to professional, geographic, and gender diversity: 46 intensivists, 6 pharmacists, 3 nurses, and 1 PhD scientist, working across 22 countries on five continents. The intensivists themselves were not a monoculture. Their training crossed intensive care, anesthesiology, internal medicine, pulmonology, cardiology, infectious diseases, and emergency medicine.
The Delphi process ran from May 13 to September 6, 2025, across five sequential rounds. The steering committee drafted 34 candidate statements covering eight clinical domains: the case for a definition itself, blood pressure targets, markers of tissue perfusion, fluid resuscitation, vasoactive therapy, adjunct therapies, source control, and the type of shock. Consensus was defined as agreement from at least 75% of panellists on the highest or lowest tiers of a seven-point Likert scale, with stability tested between consecutive rounds using a non-parametric chi-square test.
Five of the 34 statements were rejected outright after the second round. Of the 29 that survived, 13 reached the 75% consensus threshold and entered the final criteria set. Twelve more reached stability without consensus, meaning the panel reliably could not agree, and the disagreement itself became a piece of data. Reporting followed the ACCORD framework, the current standard for Delphi work in biomedicine.
A word on what this evidence is and is not. Expert consensus sits below randomized data on every formal hierarchy. The panel itself names this. For an entity that does not yet have prospective trial criteria, and arguably cannot have them because the entity has not been definable enough to study, structured consensus is the appropriate methodology. It is what we used to land Sepsis-3 in 2016. It is what we use for the Berlin Definition. It is what we use for the Global Definition of ARDS. The bar is not “is this Level 1 evidence?” The bar is “is this a defensible foundation that the field can build trials on?” The answer here is yes.
Watch the following video:
What Stood Out
Six elements of the final criteria deserve specific attention because each one is consequential at the bedside.
First, lactate without a cutoff. The panel converged at 94.6% agreement on lactate as a tissue perfusion marker, but explicitly declined to specify a cutoff value. Panellists split between 2 and 4 mmol/L, and that split is itself informative. Refractory septic shock is not a number on a meter. It is a trajectory: lactate that is not coming down despite all the standard moves.
Second, capillary refill time entered the consensus. CRT reached 76.8% agreement as a perfusion criterion. This is the element that should make every RT and bedside nurse on this Substack lean forward. CRT requires no central access, no arterial line, no point-of-care analyzer, and no fellow available at 0300. It requires a glass slide, the distal phalanx of a finger, and ten seconds of compression. The endorsement of CRT in a joint SCCM/ESICM consensus is the field formally catching up to what ANDROMEDA-SHOCK and ANDROMEDA-SHOCK-2 demonstrated: one of the simplest bedside maneuvers in resuscitation is also one of the most informative.
Third, the norepinephrine threshold is base equivalents, not “max dose.” The panel landed on greater than 0.5 µg/kg/min expressed as norepinephrine base equivalents. Not norepinephrine tartrate. Not unspecified salts. Not “max” in a flowsheet. The criterion builds on the 2024 SCCM/ESICM joint position paper from Wieruszewski and colleagues that established norepinephrine base reporting as the standard for transparency in critical care. The pharmacology matters. Norepinephrine tartrate is approximately half the base concentration of an equivalently labeled vial of norepinephrine bitartrate, and the field has been silently reporting doses inconsistently for years. The 0.5 µg/kg/min threshold presumes you and your pharmacist are on the same denominator.
Fourth, the consensus deliberately walks away from defining refractoriness by the addition of a second or third vasopressor. Total dose matters. The number of agents does not. This is a deliberate move against the practice of declaring refractoriness the moment a clinician hangs vasopressin or angiotensin II, given the rising literature on early multimodal vasopressor strategies that are themselves a feature of modern resuscitation rather than a failure.
Fifth, critical care ultrasound was the single diagnostic modality the panel endorsed at 92.9% agreement, and it was endorsed specifically to confirm or exclude mixed shock physiology. Pulmonary artery catheterization was excluded. Imaging beyond CCUS was placed in standard-of-care territory rather than refractoriness-specific territory. The takeaway for every interprofessional team is direct. If your unit does not have a credentialed CCUS pathway, that gap has now been promoted from “nice to have” to “consensus criterion of the most severe phenotype in sepsis.”
Sixth, the panel declined to include several long-cited markers, namely central venous oxygen saturation, urine output, mottling score, central venous to arterial carbon dioxide difference, and lactate clearance as a standalone target. These omissions are not oversights. ScvO2’s relationship with mortality is U-shaped in septic shock. Urine output is contaminated by diuretics, osmolar load, and chronic kidney dysfunction. Lactate clearance as a fixed percentage target has not survived the methodological scrutiny of the past five years. The panel is not saying these data points are useless. The panel is saying they are not robust enough to anchor the most consequential phenotype designation in sepsis.
Listen to the following podcast:
Physiologic, Clinical, Leadership, and Ethical Interpretation
The deeper read on this consensus is that it formalizes a shift in how critical care is conceptualizing the sickest septic patient.
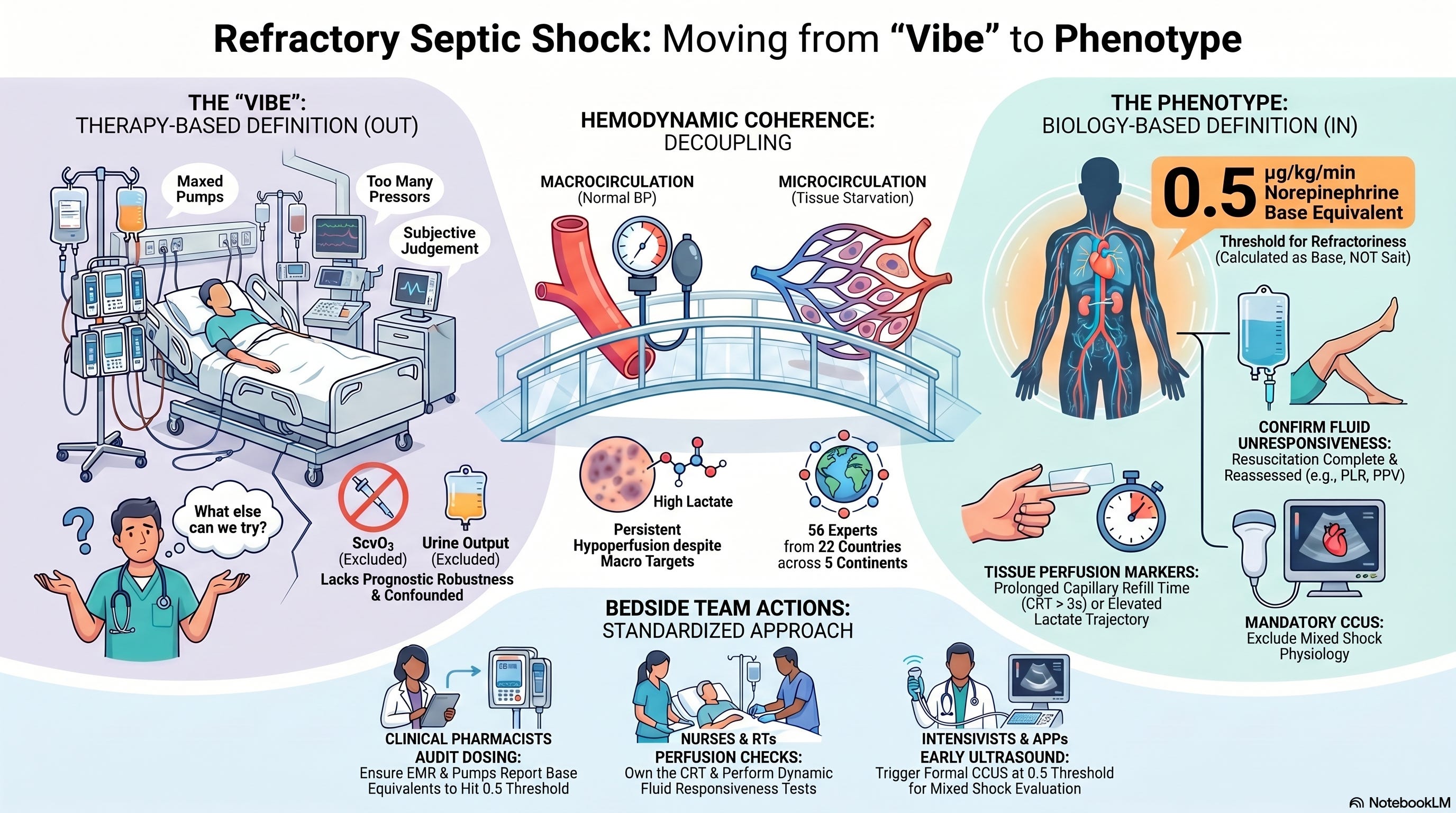
For two decades, “refractory” was defined inward, by what we had run out of. Vasopressors maxed. Fluid given. Adjuncts added. The phenotype was a residual: whatever was left after we had tried the standard moves. That framing locates refractoriness in the therapy, not in the patient.
The new criteria flip this. The phenotype is defined outward, by the patient’s biology. Persistently disturbed tissue perfusion that standard resuscitation has not corrected. Lactate and CRT are biology. Fluid unresponsiveness is biology. Vasopressor dose is a marker, but the criterion that anchors it is the patient’s continued tissue hypoperfusion at that dose. The clinician is no longer the protagonist of the definition. The patient is.
This matters for three reasons.
It matters clinically because it tells the team where to look. Once a patient meets criteria, the next question is no longer “what therapy should we add?” The next question is “is the shock still vasoplegic, or is it now mixed?” That is the question CCUS answers. The criteria are operationalizing differential diagnosis at the worst moment in the trajectory, when the team’s instinct is to escalate pharmacology and the patient’s actual need may be to add an inotrope, drain a fluid collection, or re-evaluate the source.
It matters for research because it gives the trial-design community something it has not had: a single phenotype on which to test rescue therapies that have repeatedly underperformed in all-comer septic shock populations. Angiotensin II in ATHOS-3 worked in a high-norepinephrine subgroup that was effectively this phenotype. Hydrocortisone signals shift when the population is enriched for refractoriness. Hemoadsorption, methylene blue, and selective B-cell modulators have failed in heterogeneous shock cohorts and may yet succeed when tested in the right one. The criteria make those next-generation trials possible.
It matters for the conversation we have at the bedside, with each other and with families. “Refractory septic shock” now carries weight that all six disciplines in the ICU can mean the same thing by. When the charge nurse says it, when the consulting pharmacist says it, when the resident calls the attending, when the RT requests the prone team, the words now point to the same patient.
A leadership tangent worth naming. The joint authorship is itself a model of what global critical care should look like in 2026. The SCCM, the largest critical care society on Earth, and ESICM, the dominant European voice, do not consistently move in lockstep. When they do, the field should pay attention, because joint motion is rare and costly to produce. Fifty-six panellists, five rounds, fifteen months from steering committee formation to publication. That is the actual cost of consensus. For interprofessional teams, the model is also worth absorbing. The panel deliberately included pharmacists and nurses alongside intensivists. The seat at the table mattered to the product.
Bedside / Workplace Takeaways
For the Monday morning interprofessional ICU team, six concrete shifts:
Adopt the operational language now. Refractory septic shock from this week forward should mean: a patient with septic shock, fluid unresponsive after initial resuscitation, on a norepinephrine base equivalent dose greater than 0.5 µg/kg/min, with persistently elevated lactate and/or prolonged capillary refill time, and with CCUS performed to assess for mixed shock physiology. Bring it to your unit’s morning huddle this week.
Pharmacists, audit your norepinephrine reporting. If your unit still mixes base and tartrate concentrations in the EMR without a unified denominator, you are not measuring the threshold this consensus is built on. Lead the conversation with your medication safety committee.
Respiratory therapists, your CRT assessment matters now. The bedside maneuver you can do without an order, without a line, without a lab, is in the consensus. Document it. Communicate it on rounds. The criterion exists because of perfusion data, not pressure data, and perfusion data is RT-and-nurse-collectable.
Bedside nurses, the fluid responsiveness check is yours to drive. The criterion explicitly requires reassessment of fluid responsiveness before declaring refractoriness. Passive leg raise, pulse pressure variation, end-expiratory occlusion test. These are nursing-led assessments in most modern ICUs. Own them.
Intensivists and APPs, schedule the CCUS exam. If your unit doesn’t have a structured CCUS protocol that triggers when a patient crosses 0.5 µg/kg/min of norepinephrine without perfusion correction, you have a workflow gap. The consensus has elevated CCUS from optional to expected for this phenotype.
Build the criteria into your sepsis dashboard. Whether your unit uses Epic, Cerner, MetaVision, or something else, the criteria are extractable: perfusion marker, fluid responsiveness assessment, vasopressor dose, CCUS. Make refractory septic shock a flagged phenotype, not a vibe.
Teaching Pearl
When you teach this consensus to a fellow, a new graduate RT, a charge nurse running orientation, or a pharmacy resident on ICU rotation, anchor it to a single physiologic concept: hemodynamic coherence. The idea, popularized by Can Ince and now embedded in every modern sepsis curriculum, is that macrocirculation and microcirculation can decouple. A patient can have a MAP of 70, a cardiac index of 3.2, and a urine output of 0.8 mL/kg/hr, and still have a knee that mottles, a finger that refills sluggishly, and a lactate that climbs.
That decoupling is what refractory septic shock looks like physiologically. The consensus does not invent the concept. It operationalizes it. Persistently disturbed perfusion despite met macrocirculatory targets, on a vasopressor dose that should be enough. That is microcirculatory failure, and that is the phenotype the criteria capture. Teach this and the criteria will make sense. Skip this and the criteria will feel like a checklist.
What We Should Not Over-Assume
Three honest concerns the field should hold alongside the criteria.
First, this is consensus, not prospective validation. The 13 criteria are defensible. They are not yet proven to identify the right patients for the right interventions. The next five years should produce validation cohorts, ideally embedded in the SSC registry network, that test whether patients meeting these criteria actually have the outcomes and respond to the rescue therapies the consensus implies. Until that work is in, the criteria are a framework, not an oracle.
Second, the 0.5 µg/kg/min threshold is acknowledged by the panel itself as resting on weak evidence. It reflects the median of the published literature, not a prospectively derived inflection point. There is no biological reason 0.49 µg/kg/min is a different patient than 0.51. The threshold is a useful operational anchor. It is not a physiologic truth.
Third, the criteria do not address pediatric septic shock, do not address post-cardiotomy mixed shock, and do not specify duration of failure. The panel tried to specify a time window and could not reach consensus. A patient who has been on 0.55 µg/kg/min for thirty minutes is, by these criteria, the same patient as one who has been on it for six hours. That is a gap the next iteration will have to close.
Limitations
The acknowledged limitations are real and worth naming. Delphi methodology, by definition, generates expert opinion under structured conditions. It is not a prospective study. The panel was multinational but skewed toward academic centers, which may limit generalizability to community ICUs where some of these criteria (CCUS in particular) are not universally available. The panel composition included only three nurses, six pharmacists, and zero respiratory therapists in a denominator of 56. That is a representation gap future iterations should close, given that nursing, RT, and pharmacy bedside data are the operational backbone of every criterion in the final set. Conflicts of interest were disclosed and adjudicated through the organising societies, but several panellists carry industry relationships across the vasopressor and adjunct-therapy space that the field should keep in mind when reading the dose-specific criteria. None of these limitations invalidate the consensus. They define its boundaries.
Bottom Line
Refractory septic shock, after thirty years of clinical use without operational definition, now has 13 consensus-based criteria endorsed by the two largest critical care societies in the world. The bedside-ready synthesis is this: persistently elevated lactate and/or prolonged capillary refill time, in a patient with septic shock who is fluid unresponsive, on a norepinephrine base equivalent dose greater than 0.5 µg/kg/min, with critical care ultrasound to assess for mixed shock. Bring it to your unit’s huddle this week. The phrase is no longer a feeling. It is a phenotype.
Reference
Leone M, Myatra SN, Dugar S, et al. Clinical criteria for the definition of refractory septic shock: a joint Delphi consensus from the Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM). Intensive Care Med. 2026. doi:10.1007/s00134-026-08344-2
Leone M, Myatra SN, Dugar S, et al. Clinical Criteria for the Definition of Refractory Septic Shock: A Joint Delphi Consensus from the Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM). Crit Care Med. 2026. doi:10.1097/CCM.0000000000007124
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801 to 810. doi:10.1001/jama.2016.0287
Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49(11):e1063 to e1143. doi:10.1097/CCM.0000000000005337
Coopersmith CM, Prescott HC, Azevedo LCP, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026. Crit Care Med. 2026. doi:10.1097/CCM.0000000000007075
Hernandez G, Ospina-Tascón GA, Damiani LP, et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA. 2019;321(7):654 to 664. doi:10.1001/jama.2019.0071
ANDROMEDA-SHOCK-2 Investigators; Hernandez G, Ospina-Tascón GA, Kattan E, et al. Personalized Hemodynamic Resuscitation Targeting Capillary Refill Time in Early Septic Shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial. JAMA. Published online October 29, 2025. doi:10.1001/jama.2025.20402
Antonucci E, Polo T, Giovini M, et al. Refractory septic shock and alternative wordings: a systematic review of literature. J Crit Care. 2023;75:154258. doi:10.1016/j.jcrc.2023.154258
Wieruszewski PM, Leone M, Kaas-Hansen BS, et al. Position Paper on the Reporting of Norepinephrine Formulations in Critical Care From the Society of Critical Care Medicine and European Society of Intensive Care Medicine Joint Task Force. Crit Care Med. 2024;52(4):521 to 530. doi:10.1097/CCM.0000000000006176
Kotani Y, Di Gioia A, Landoni G, et al. An updated “norepinephrine equivalent” score in intensive care as a marker of shock severity. Crit Care. 2023;27(1):29. doi:10.1186/s13054-023-04322-y
Monnet X, Messina A, Greco M, et al. ESICM guidelines on circulatory shock and hemodynamic monitoring 2025. Intensive Care Med. 2025;51:1971 to 2012. doi:10.1007/s00134-025-08023-8
Mekontso Dessap A, AlShamsi F, Belletti A, et al. European Society of Intensive Care Medicine (ESICM) 2025 clinical practice guideline on fluid therapy in adult critically ill patients: part 2, the volume of resuscitation fluids. Intensive Care Med. 2025;51:461 to 477.
Diaz-Gomez JL, Sharif S, Ablordeppey E, et al. Society of Critical Care Medicine Guidelines on Adult Critical Care Ultrasonography: Focused Update 2024. Crit Care Med. 2025;53:e447 to e458.
Ince C. Hemodynamic coherence and the rationale for monitoring the microcirculation. Crit Care. 2015;19(Suppl 3):S8. doi:10.1186/cc14726
Khanna A, English SW, Wang XS, et al. Angiotensin II for the Treatment of Vasodilatory Shock. N Engl J Med. 2017;377(5):419 to 430. doi:10.1056/NEJMoa1704154
Francois B, Shi R, Teboul JL. Refractory septic shock new definition: a first stone to pave a long way. Intensive Care Med. 2026. [Editorial accompanying Leone et al.]
Clinical Disclaimer
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.