

The Conservative Oxygen Hypothesis Is Dead. The Lesson Isn’t.

After UK-ROX added 16,500 patients to a literature already pointing in one direction, the trial-grade verdict on conservative oxygenation targets in unselected ICU adults is now unambiguous. The harder question is what twenty years of well-intentioned physiologic reasoning ahead of trial evidence cost the field, and what should change in how the next hypothesis gets adopted.
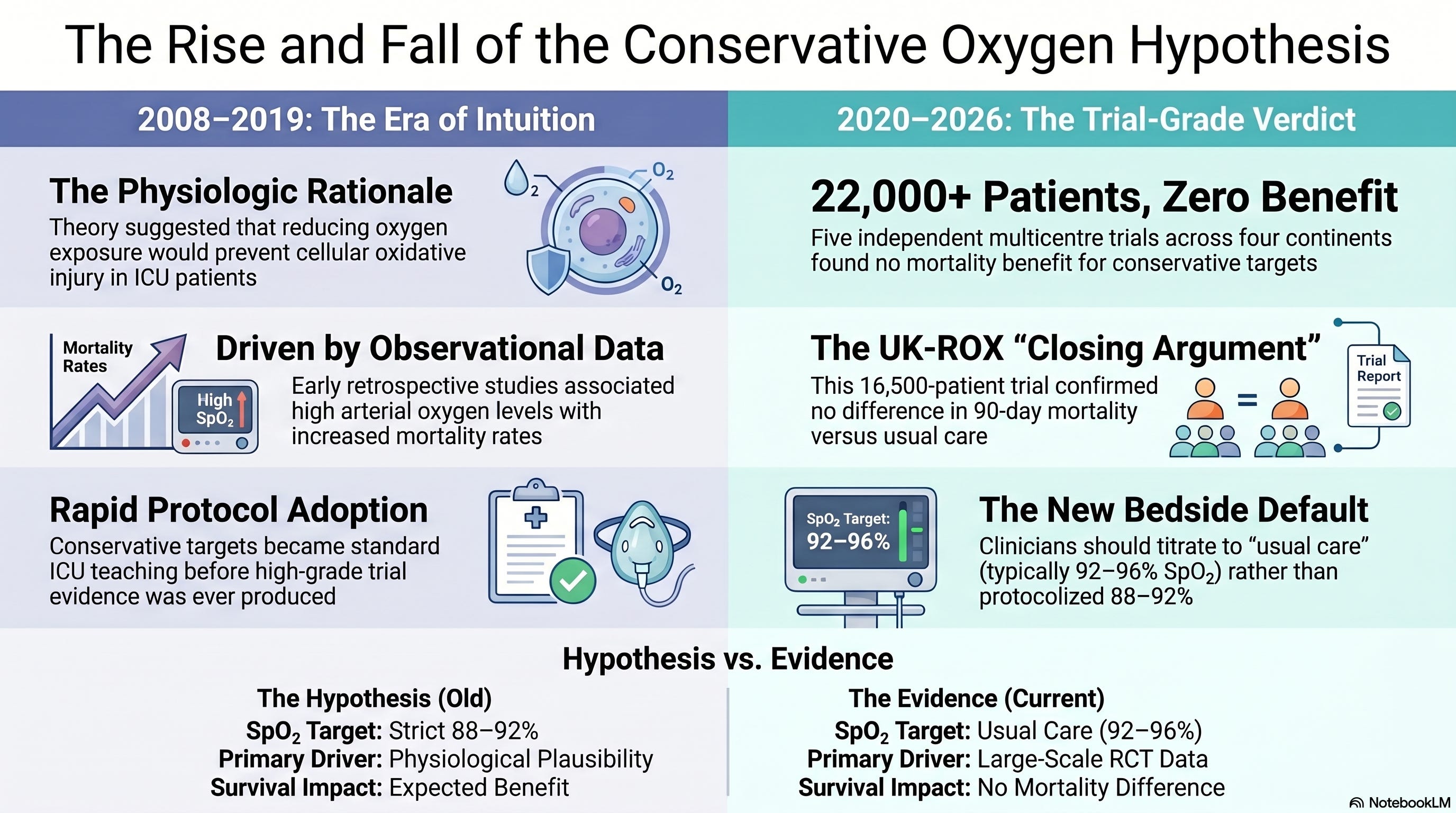
For two decades, the conservative oxygenation hypothesis lived comfortably at the intersection of physiologic plausibility, observational signal, and good intentions. Hyperoxia causes oxidative injury in cell-culture systems. Supraphysiologic arterial oxygen tensions are associated with mortality in retrospective ICU cohorts. The intuition that less oxygen exposure must, on net, mean less harm was easy to hold and easier to teach. By the time the trials began arriving in 2020, the conservative-oxygen mental model was already embedded in protocol committees, fellowship lectures, and the standing orders of more units than anyone had counted. And then the trials kept coming back negative. With UK-ROX, published in JAMA in 2025, the trial evidence is no longer ambiguous. The conservative-oxygen hypothesis, as a population-level intervention in unselected mechanically ventilated adults, is closed. The lesson the field should take from how it got here is the more important story.
Why This Matters
The conservative-oxygenation arc is the most expensive methodological cautionary tale of the last decade of critical care. Tens of thousands of patients were randomised across multiple continents because a hypothesis built on physiology and observational data was adopted as practice before trial evidence existed to support it. The trials have now been done, the verdict is consistent, and the verdict does not vindicate the hypothesis. The reason this matters beyond the SpO₂ number is that the field is currently doing the same thing — adopting physiologically attractive hypotheses ahead of trial evidence — across at least a dozen other live questions in the ICU. Clinicians who internalise what went wrong with conservative oxygenation will be measurably better at reading the next hypothesis that is built the same way. Clinicians who treat UK-ROX as a single trial result rather than the closing argument in a twenty-year case will be set up to repeat the cycle.
The Core Argument
Three statements can be defended simultaneously. First: the conservative-oxygenation hypothesis, as a strategy of targeting an SpO₂ near 90% (range 88–92%) in unselected mechanically ventilated ICU adults, does not reduce mortality compared with usual care, and the trial evidence on this point is now overwhelming and consistent across populations, geographies, and trial designs. Second: this does not mean oxygen titration is unimportant; profound hyperoxia is biologically harmful, profound hypoxemia is acutely harmful, and the bedside titration of FiO₂ to a reasonable target range remains good practice. Third: the most important lesson is methodological — the field adopted a population-level protocol change based on physiologic reasoning and observational data, found that the population-level trial evidence did not support it, and should now be more cautious about how the next intuition-rich hypothesis is incorporated into protocols. The next conservative-oxygenation-shaped mistake is already being made somewhere on a unit-level practice committee this week.
What the Evidence Shows
The conservative-oxygenation hypothesis began with observational data — de Jonge and colleagues in 2008, Palmer and colleagues in 2019, and a substantial intervening literature suggesting that supraphysiologic arterial oxygen tensions tracked with worse outcomes in mechanically ventilated ICU patients. (1,2) An influential 2018 meta-analysis, the IOTA review, suggested mortality benefit from conservative oxygenation across acute illness, and the conservative-oxygen mental model entered teaching curricula at a speed that, in retrospect, the underlying evidence did not justify.
The trial-grade evidence began arriving in 2020. ICU-ROX, the binational Australian–New Zealand trial of one thousand mechanically ventilated adults randomised to conservative versus usual oxygen, found no difference in ventilator-free days and no mortality benefit. (3) HOT-ICU, a Danish-led trial of 2,928 adults with acute hypoxemic respiratory failure, compared a PaO₂ target of 60 mm Hg with 90 mm Hg and found no difference in 90-day mortality. (4) PILOT, a single-centre US trial of more than 2,500 mechanically ventilated patients randomised across three SpO₂ target ranges, found no mortality difference and no difference in ventilator-free days. (5) The BOX trial in 2022 tested conservative versus liberal oxygenation specifically in comatose survivors of out-of-hospital cardiac arrest — a population in whom the conservative hypothesis had the strongest theoretical footing — and found no difference in death or severe disability at 90 days. (6)
The 2024 individualised-treatment-effects analysis by Bray and colleagues, published in JAMA, was the most methodologically sophisticated effort to find the patient subgroups in whom conservative or liberal targets might differ. Across pooled data from ICU-ROX, HOT-ICU, and PILOT, the analysis found no clinically meaningful subgroup-specific signal. (7) The 2025 TRAUMOX2 trial tested early restrictive versus liberal oxygenation in trauma patients and found no difference in 30-day mortality or major complications. (8)
UK-ROX, published in JAMA in 2025, is the trial that closes the argument at the population level. (9) Across 97 ICUs in the United Kingdom, 16,500 mechanically ventilated adults receiving supplemental oxygen were randomised to either conservative oxygen therapy (lowest FiO₂ to maintain SpO₂ at 90%) or usual oxygen therapy at clinician discretion, between May 2021 and November 2024. Ninety-day all-cause mortality was 35.4% in the conservative group and 34.9% in the usual-care group — no statistically significant difference. The trial was powered to detect a 2.5% absolute mortality difference, and the observed difference did not approach that threshold. With UK-ROX added to the prior literature, the population-level signal is consistent across more than 22,000 randomised patients in five independent multicentre trials spanning four continents.
The 2026 OXY-BREATHES systematic review and meta-analysis by Aljazeeri, published in Critical Care Medicine, synthesises the available evidence to the same conclusion: no mortality benefit to conservative oxygenation in mechanically ventilated ICU adults. (10) The Mega-ROX research program — a 40,000-patient registry-embedded trial program with nested RCTs in hypoxic-ischaemic encephalopathy post-cardiac arrest, sepsis, and non-HIE acute brain injury — remains the open question for whether identifiable subgroups exist in whom the answer differs from the population. (11) That question is empirically reasonable and is being addressed; it does not change the population-level verdict that is now established.
Watch the following video:
Interpretation
Two readings of this literature are wrong, and they are wrong in opposite directions. The first wrong reading is to dismiss the trials. “These trials were imperfect” is technically true of every trial ever conducted and operationally true of nothing. The conservative-oxygenation hypothesis received as fair a hearing across as many populations and study designs as the field has ever granted any single ICU question. The trials separated the two strategies adequately, were powered appropriately, were conducted across diverse health systems, and converged on the same answer. A clinician who continues to assert that conservative oxygenation reduces mortality in unselected ICU adults is, at this point, asserting a position the trial evidence does not support.
The second wrong reading is to use UK-ROX as license to wander toward hyperoxia. The trial-grade evidence shows no harm from a usual-care strategy that, in most ICUs, results in SpO₂ ranges modestly higher than the conservative target. It does not show that pushing FiO₂ to unnecessarily high levels is benign. The observational signal of hyperoxia harm, while inadequate to justify the population-level protocol change the field made, is not nothing — biologically implausible to ignore, even if trial-grade not strong enough to invert practice. The reasonable bedside default is to titrate FiO₂ to a target range that avoids both clinically significant hypoxemia and unnecessary supraphysiologic exposure, which is what most clinicians have always done and what the trials describe as “usual care.”
The methodological reading is the more important one. The field adopted a population-level practice change — narrowed SpO₂ targets, protocols nudged toward the lower end of acceptable ranges, fellowship teaching pivoted — based on a combination of physiologic reasoning, observational data, and a meta-analysis whose primary studies were heterogeneous in ways that turned out to matter. The trials that should have preceded the practice change followed it instead, and consistently failed to validate the hypothesis. The cost of getting this wrong is not catastrophic — no mass mortality signal in either direction — but it is real: thousands of patient-hours managed under a protocol that was never trial-validated, an educational generation taught a hypothesis as if it were established knowledge, and a substantial international research investment to clean up the resulting question. The field should not pretend this was a victimless cycle.
The connection to Friday’s pulse-oximetry coverage is worth drawing here. The conservative-oxygenation target of SpO₂ 88–92% sits exactly in the range where pulse-oximeter performance is most variable across patients with darker skin pigmentation — the zone where overestimation of true arterial saturation is most likely to result in occult hypoxemia. To the extent the conservative-oxygenation strategy was being implemented in patients whose pulse-oximeter readings could not be fully trusted in that range, the strategy was even more poorly grounded for those patients specifically than for the population as a whole. UK-ROX did not specifically address this interaction, and no oxygenation-target trial yet has stratified by skin pigmentation. The next generation of these trials should.
Bedside / Workplace Application
Update the protocol. Units that adopted a conservative-oxygenation protocol based on the pre-2020 literature should now reconsider it. The trial-grade evidence supports a usual-care approach — titrate FiO₂ to a clinically reasonable target range, neither aggressively pushing toward the lower end nor permitting unnecessary supraphysiologic exposure. A specific number is less important than the abandonment of the protocolised pursuit of 88–92%.
Update the teaching. Fellowship curricula, RT certification reviews, and ICU orientation materials that present conservative oxygenation as evidence-based practice should be revised. The conservative-oxygen hypothesis is now a history-of-the-field topic, not a clinical recommendation.
Do not over-correct toward hyperoxia. The trial evidence does not validate hyperoxia. Routine FiO₂ above what the patient’s clinical state requires is not what the trials studied and not what they support. The default remains lowest FiO₂ that maintains a reasonable SpO₂ range — usually 92–96% for most patients, with documented exceptions for specific conditions (chronic CO₂ retainers, paraquat exposure, bleomycin history, and so on).
Watch the pulse oximeter especially carefully in patients with darker pigmentation. Targets near 88–92% are particularly fraught in this population because of the asymmetric measurement error documented in the 2020–2026 pulse-oximetry literature. Where targets in the lower acceptable range are used at all, additional bedside scepticism and a lower threshold for arterial blood gas confirmation are warranted.
For research-active units: Mega-ROX subgroups are the open question. The HIE-post-cardiac-arrest, sepsis, and non-HIE acute-brain-injury nested RCTs remain potentially practice-shaping. The population-level answer is settled; the subgroup-level question is not.
Teaching Pearl
The single concept worth teaching from the conservative-oxygenation arc is the gap between mechanism-based plausibility and population-level efficacy. Hyperoxia genuinely is biologically harmful at the cellular level; oxidative injury is real; the observational signal was real. None of those statements is enough to support a population-level practice change. The translation from mechanism to protocol requires intermediate evidence that the mechanism actually drives clinically meaningful outcomes in real ICU populations at the doses and durations being studied, and that evidence requires trials. Fellowship learners who internalise this gap — who can hold “the mechanism is real” and “the population-level intervention does not work” as simultaneously true without resolving the tension by collapsing one — will be substantially better readers of every future clinical hypothesis built on the same template, including the AI-augmented and precision-medicine hypotheses currently being marketed.
Listen to the following podcast:
Over-Assumptions
The first over-assumption to watch for is the slide from “no population-level signal” to “no signal anywhere.” Mega-ROX is testing specific subgroups precisely because the field cannot exclude the possibility that identifiable populations exist in whom oxygenation targets matter. That work is ongoing and should be respected. The second is the inverse — the assumption that because some signal might still emerge in a subgroup, the population-level practice change can be maintained. It cannot. The default for unselected patients is now usual care, and any subgroup-specific deviation needs its own trial evidence. The third is the assumption that the methodological lesson is unique to oxygenation. It is not. Several other current ICU protocols — including some that touch ventilation strategy, fluid management, and sedation depth — are running on the same physiology-plus-observation footing the conservative-oxygenation hypothesis was. The conservative-oxygenation story is a template, not a one-off.
Limitations
This piece synthesises across heterogeneous trial designs, populations, and oxygenation targets. The trials cited used somewhat different conservative-arm definitions (PaO₂ 60 mm Hg in HOT-ICU; SpO₂ 90% in UK-ROX; multiple SpO₂ ranges in PILOT), and direct head-to-head comparison of strategies requires careful attention to those differences. The population-level conclusion that conservative oxygenation does not reduce mortality is robust across that heterogeneity; finer-grained conclusions about specific oxygen-target ranges are less so. Generalisability to populations underrepresented in the trial portfolio — including paediatric ICU patients, very high-altitude ICU practice, and post-operative cardiothoracic populations with their own oxygen-handling considerations — is an empirical question this synthesis does not resolve. The interaction with pulse-oximetry measurement bias is raised here as a methodological concern, not as a result; no oxygenation-target trial to date has stratified by skin pigmentation, and the interaction effect is hypothesis-generating rather than established.
Bottom Line
The conservative-oxygenation hypothesis is closed by trial evidence at the population level. The methodological lesson — that mechanism-based plausibility and observational signal are insufficient to drive population-level practice changes without trial validation — is the more durable contribution of the entire research program. Update the protocol. Update the teaching. Watch for the next hypothesis built on the same template. The field should be better at this by now, and it is the editorial task of every clinical-intelligence publication, this one included, to insist that it become so.
References
de Jonge E, Peelen L, Keijzers PJ, et al. Association between administered oxygen, arterial partial oxygen pressure and mortality in mechanically ventilated intensive care unit patients. Crit Care. 2008;12(6):R156. doi:10.1186/cc7150
Palmer E, Post B, Klapaukh R, et al. The association between supraphysiologic arterial oxygen levels and mortality in critically ill patients: a multicenter observational cohort study. Am J Respir Crit Care Med. 2019;200(11):1373-1380.
ICU-ROX Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group; Mackle D, Bellomo R, Bailey M, et al. Conservative oxygen therapy during mechanical ventilation in the ICU. N Engl J Med. 2020;382(11):989-998. doi:10.1056/NEJMoa1903297
Schjørring OL, Klitgaard TL, Perner A, et al; HOT-ICU Investigators. Lower or higher oxygenation targets for acute hypoxemic respiratory failure. N Engl J Med. 2021;384(14):1301-1311.
Semler MW, Casey JD, Lloyd BD, et al; PILOT Investigators. Oxygen-saturation targets for critically ill adults receiving mechanical ventilation. N Engl J Med. 2022;387(19):1759-1769.
Schmidt H, Kjaergaard J, Hassager C, et al. Oxygen targets in comatose survivors of cardiac arrest. N Engl J Med. 2022;387(16):1467-1476. doi:10.1056/NEJMoa2208686
Bray J, Skrifvars MB, Casey JD, et al. Individualized treatment effects of oxygen targets in mechanically ventilated critically ill adults. JAMA. 2024;331(14):1195-1204. doi:10.1001/jama.2024.2933
Arleth T, Baekgaard J, Siersma V, et al. Early restrictive vs liberal oxygen for trauma patients: the TRAUMOX2 randomized clinical trial. JAMA. 2025;333(6):479-489. doi:10.1001/jama.2024.25786
Martin DS, Gould DW, Shahid T, et al; UK-ROX Investigators. Conservative oxygen therapy in mechanically ventilated critically ill adult patients: the UK-ROX randomized clinical trial. JAMA. 2025;334(5):398-408. doi:10.1001/jama.2025.9663
Aljazeeri J. Conservative oxygen targets in mechanically ventilated patients (OXY-BREATHES): a systematic review and meta-analysis of randomized controlled trials. Crit Care Med. 2026. doi:10.1097/CCM.0000000000007031
Young PJ, Arabi YM, Bagshaw SM, et al; Mega-ROX Management Committee. Protocol and statistical analysis plan for the Mega Randomised Registry Trial research program comparing conservative versus liberal oxygenation targets in adults receiving unplanned invasive mechanical ventilation in the ICU (Mega-ROX). Crit Care Resusc. 2022;24(2):137-149.
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.