

The Lung at Rest
VV-ECMO, Ultraprotective Ventilation, and the Honest Limits of the 2026 Evidence in Severe ARDS

For six Tuesdays at ICCN I have written about the variables the ventilator screen does not show, and the bedside tools that make them visible. Drive in the P-SILI piece. The post-extubation bridge. Transpulmonary pressure through esophageal manometry. Diaphragm function through ultrasound. The closed loop of neural drive through NAVA. Each one is a way to protect the lung more precisely while the patient is still on the ventilator. This week’s piece is about the moment when all of that is not enough. When the lung is so injured that no combination of tidal volume, PEEP, prone positioning, paralysis, and drive control can keep it safe. The escape hatch from that situation is venovenous extracorporeal membrane oxygenation, and the honest story of what it can and cannot promise is more interesting, and more contested, than the enthusiasm around it usually admits.
Why This Matters
The logic of VV-ECMO is mechanically clean. An injured lung needs gas exchange, and gas exchange on a conventional ventilator requires moving air in and out with pressures and volumes that can themselves injure the lung. This is the central paradox of severe ARDS. The treatment is part of the disease. VV-ECMO breaks the paradox by moving gas exchange outside the body. Venous blood is drained, pumped across a membrane that adds oxygen and removes carbon dioxide, and returned to a central vein. With the membrane doing the work, the ventilator can be turned down to settings that apply far less mechanical force to the lung. Lower tidal volume. Lower plateau pressure. Lower driving pressure. The lung, in the language clinicians use, is put at rest.
That mechanical claim is real and well-documented. What happens next, whether resting the lung this way actually saves more lives, is where the evidence becomes genuinely uncertain, and where an honest publication has to slow down.
For the interprofessional team this matters because VV-ECMO is the most resource-intensive, highest-risk, and most expensive intervention in the respiratory failure toolkit. It commits a patient to systemic anticoagulation, large-bore cannulas, a circuit that can fail, and a constellation of bleeding and thrombotic risks. The decision to start it, and the decisions about how to ventilate the lung once it is running, are made by a team in which the perfusionist, the intensivist, the respiratory therapist, the nurse, the pharmacist, and the APP each hold a piece that no one else can supply. Getting the evidence right is what keeps that team from offering a patient a hard therapy with a soft justification.
The Study / Evidence in Context
There is no single anchor trial for this article, because the honest version of this topic is a conversation among several trials that do not fully agree. The team needs all of them.
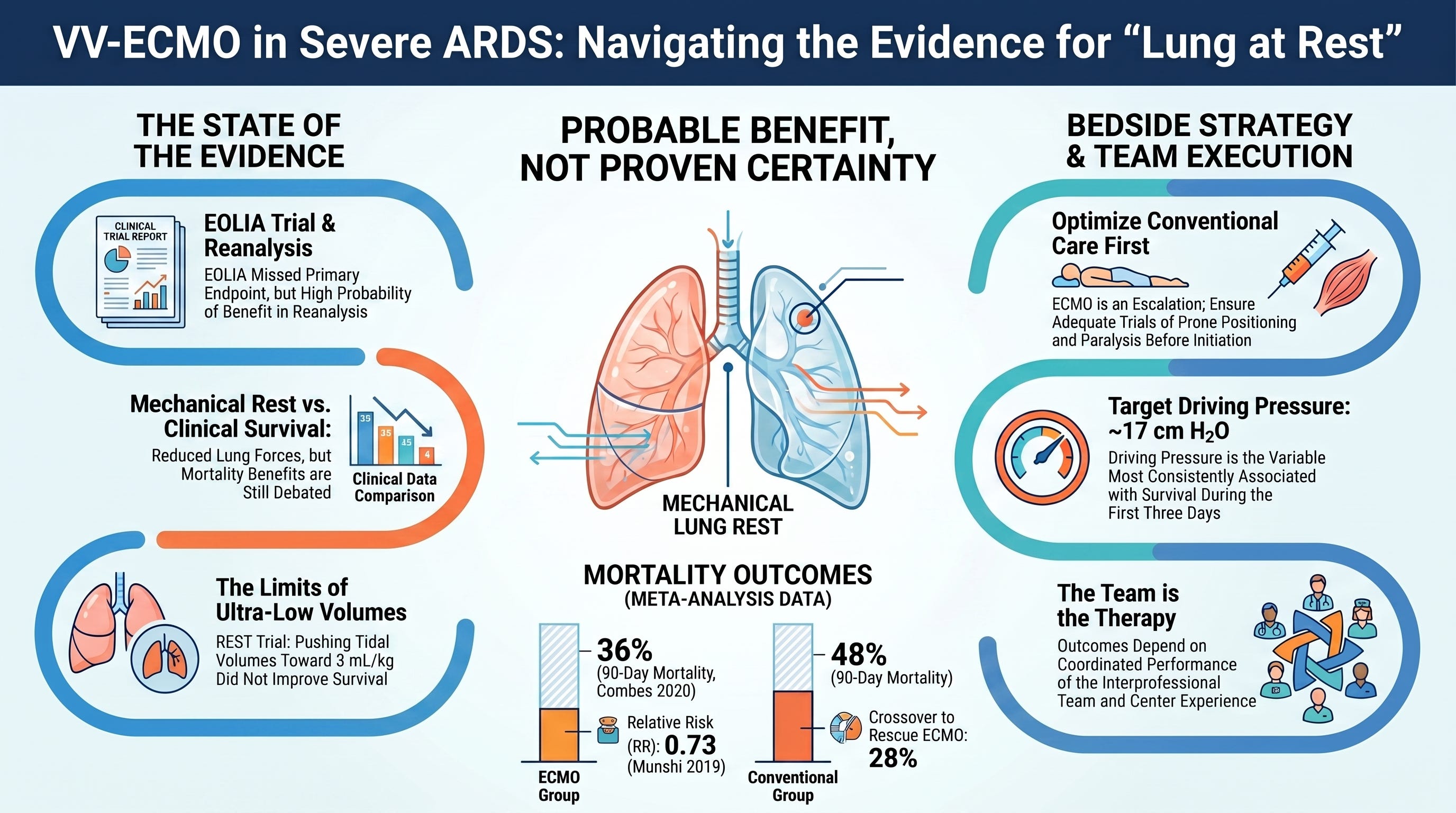
The central trial is EOLIA, published by Combes and colleagues in 2018. It randomized 249 patients with very severe ARDS to early VV-ECMO or to a protocolized conventional ventilation strategy that allowed crossover to rescue ECMO for refractory hypoxemia. The result that matters most is the one most often glossed over. EOLIA did not meet its primary endpoint. Sixty-day mortality was 35% in the ECMO group and 46% in the control group, a relative risk of 0.76 with a 95% confidence interval of 0.55 to 1.04 and a p-value of 0.09. The trial was stopped early for meeting a prespecified futility boundary. By the strict reading that the trialists themselves applied, early ECMO did not significantly reduce mortality compared with a conventional strategy that included rescue ECMO.
Two features complicate that negative reading, and both are legitimate. First, 28% of the control group crossed over to rescue ECMO at a mean of 6.5 days, because they were dying without it. That crossover narrows the gap between the groups and makes the comparison less a test of ECMO versus no ECMO than a test of early ECMO versus delayed ECMO. Second, a prespecified secondary endpoint of treatment failure, defined as death in the ECMO group and death or crossover in the control group, did favor early ECMO significantly. These are reasons the conversation did not end in 2018.
The conversation continued through reanalysis. Goligher and colleagues published a post-hoc Bayesian reanalysis of EOLIA in JAMA later in 2018. Using a range of prior assumptions, they found a high posterior probability that early ECMO reduces mortality. Even under a strongly skeptical prior, equivalent to having data from a hypothetical trial larger than EOLIA showing no effect, the posterior probability of any mortality benefit was around 88%, rising toward 96% under more neutral priors. This is a genuinely useful way to read an underpowered trial, and it is also a reanalysis whose conclusion depends on the prior the analyst chooses, which is the standard and fair criticism of the Bayesian approach.
Two meta-analyses followed. Munshi and colleagues, in The Lancet Respiratory Medicine in 2019, pooled the two randomized trials of the modern era, CESAR and EOLIA, across 429 patients and found a 60-day mortality risk ratio of 0.73 (95% CI 0.58 to 0.92) favoring ECMO. Combes and colleagues, in an individual-patient-data meta-analysis in Intensive Care Medicine in 2020, combined the same two trials and found 90-day mortality of 36% with ECMO versus 48% with conventional management, a risk ratio of 0.75 (95% CI 0.6 to 0.94, p=0.013). Both are real signals. Both rest on only two RCTs, one of which is CESAR, a 2009 trial criticized because only 76% of the referred patients actually received ECMO and the control arm did not standardize lung-protective ventilation. A separate reanalysis by Moran and colleagues argued that the small number of trials leaves no certainty about efficacy. This is the state of the evidence. Probable benefit in expert hands in selected patients, not proof.
The second strand of this article is the ventilation strategy once ECMO is running, and here the evidence is humbling in a different way.
The appealing idea is that if ECMO lets you turn the ventilator down, you should turn it down a long way. Push the tidal volume below the conventional 6 mL/kg, toward 3 or 4 mL/kg, and minimize the mechanical forces as far as the circuit allows. This is ultraprotective ventilation. The SUPERNOVA study by Combes and colleagues in 2019 tested whether extracorporeal carbon dioxide removal could make this feasible in moderate ARDS, and it could. Around 78% of patients reached the ultraprotective target by 8 hours and 82% by 24 hours. But SUPERNOVA was explicitly a feasibility study, and its authors said plainly that a randomized trial was required to know whether it helps or harms.
That randomized trial, in effect, was REST. McNamee and colleagues, in JAMA in 2021, randomized 412 patients with acute hypoxemic respiratory failure to extracorporeal carbon dioxide removal to facilitate a tidal volume near 3 mL/kg, or to standard lung-protective ventilation. The result should anchor every clinician’s enthusiasm. Lower tidal volume facilitated by the device did not reduce 90-day mortality, and it was associated with a higher rate of serious adverse events, including intracranial hemorrhage in 2.5% of the device group. The unadjusted hazard ratio for death was 1.1. The strategy of pushing the lung to ultra-low tidal volumes using extracorporeal support, in this trial, did not help and may have harmed.
The third strand is observational, and it is where the most actionable bedside guidance currently lives. Serpa Neto and colleagues, in a pooled individual-patient analysis of 545 patients across nine studies in 2016, found that driving pressure during the first three days on ECMO was independently associated with in-hospital mortality, with an adjusted hazard ratio of 1.06 per cm H2O (95% CI 1.03 to 1.10). Survivors had a mean driving pressure around 17 cm H2O and non-survivors around 19. The LIFEGARDS cohort by Schmidt and colleagues, 350 patients across 23 experienced centers in 2019, documented that ultraprotective ventilation is widely adopted on ECMO and described its association with longer-term outcomes. These are associations, not proof of causation, and they are the best bedside signal the field currently has.
What Stood Out
A few things from this body of evidence should reorganize how the interprofessional team thinks about ECMO and the lung.
First, the headline most people carry about EOLIA is wrong. Many clinicians remember EOLIA as the trial that proved ECMO works in severe ARDS. It is more accurate to say EOLIA failed to prove it, and that the subsequent reanalyses and meta-analyses make a probabilistic case for benefit that reasonable experts still debate. The distinction matters at the bedside because it changes how the team frames the decision with a family. The honest framing is that ECMO is a reasonable, guideline-endorsed option in selected very severe ARDS at experienced centers, with probable but not proven mortality benefit, not a therapy with a settled survival advantage.
Second, more extracorporeal support is not automatically better lung protection. The intuition that pushing tidal volume ever lower must help is exactly what REST tested and did not confirm. The strategy of ultra-low tidal volume facilitated by carbon dioxide removal carries its own hazards, and at least in the population REST studied, the harms were real and the benefit was absent. This is a powerful reminder that physiologic plausibility and patient outcome are different things.
Third, driving pressure is the variable the data point to during ECMO. Of all the ventilator settings studied on ECMO, driving pressure shows the most consistent association with survival. This connects ECMO to the broader ARDS literature, where Amato and colleagues showed in 2015 that driving pressure was the ventilator variable most strongly associated with survival. On ECMO, as off it, the association between lower driving pressure and better outcome is the signal worth attending to, while remembering that association is not the same as a proven target.
Fourth, the lung-rest concept is mechanistically sound even where the outcome data are unsettled. ECMO genuinely does reduce the mechanical forces applied to the lung. Tidal volume, plateau pressure, and driving pressure all fall when ECMO is initiated, across every cohort that has measured them. The physiologic rationale for why this should reduce ventilator-induced lung injury is coherent. The honest position is that the mechanism is real and the proof that it changes mortality, beyond the contested ECMO-versus-conventional question, is not yet in hand.
Fifth, this is the most team-dependent therapy in the respiratory toolkit. EOLIA’s favorable safety profile, including a low rate of hemorrhagic stroke, was attributed by the investigators partly to experienced centers using careful, low-intensity anticoagulation. The outcome of ECMO depends heavily on the team running it. This is not a therapy where the device does the work and the team watches. The team is the therapy.
The honest version of ECMO is more useful than the enthusiastic one. A hard therapy deserves a clear-eyed account of what the evidence does and does not support.
Physiologic, Clinical, Leadership, or Ethical Interpretation
Here is my read.
VV-ECMO occupies a strange place in critical care. It is simultaneously one of the most dramatic therapies we have and one of the least definitively proven. That combination creates a temptation to let the drama stand in for the proof. A patient on ECMO looks rescued. The oxygen saturation climbs, the ventilator comes down, the immediate crisis resolves. It is easy to move from that visible improvement to a confident belief that the therapy is saving lives, when the trial evidence for a mortality benefit is probable but contested, and when the strategy of maximal lung rest through ultra-low tidal volume has actually failed in a randomized trial.
The discipline this demands is the same discipline this whole arc has been about. Distinguish what is demonstrated from what is hoped. ECMO demonstrably reduces the mechanical forces on the lung. ECMO is a reasonable, guideline-endorsed option in selected very severe ARDS. The mortality benefit is probable in expert hands and still debated. The ultraprotective strategy is feasible but not outcome-proven and, pushed to its extreme with carbon dioxide removal, was negative and possibly harmful in REST. Holding all of those statements at once is harder than carrying a simple story, and it is the only honest position.
For the interprofessional team this maps onto a workflow.
The perfusionist is the central discipline for ECMO, and this is the article where that role moves to the front. The perfusionist manages the circuit, the blood flow, the sweep gas that controls carbon dioxide removal, the membrane function, and the early recognition of circuit complications. The rate at which carbon dioxide is removed after cannulation matters, because rapid correction of hypercapnia has been associated with neurologic complications, which means the perfusionist and the intensivist titrate sweep gas together rather than maximally. The perfusionist who manages the circuit conservatively and communicates membrane performance to the team is doing safety-critical work that no other discipline can do.
The intensivist owns the candidacy decision and the escalation timing. The honest framing of the evidence changes how this decision is made. The patient with very severe ARDS who is failing conventional therapy including prone positioning and neuromuscular blockade is a reasonable candidate for ECMO consideration at an experienced center, and the intensivist who refers early, before multi-organ failure accrues, is acting on the most defensible reading of EOLIA. The intensivist also sets the lung-rest ventilation strategy and resists the temptation to push tidal volume to extremes that REST did not support.
The respiratory therapist manages the ventilator once ECMO is running, and the target is lung rest with attention to driving pressure rather than a race to the lowest possible tidal volume. The RT who keeps driving pressure low, maintains modest PEEP, and avoids both the over-distension of aggressive settings and the de-recruitment of near-apneic settings is applying the observational evidence sensibly. The RT also coordinates with the perfusionist, because the ventilator and the circuit together determine the patient’s gas exchange, and a change in one requires awareness of the other.
The nurse is the continuous bedside surveillance for the ECMO patient, watching for cannula site bleeding, circuit changes, signs of recirculation, neurologic changes, and the constellation of complications that make ECMO high-risk. The nurse is the discipline most likely to catch the early bleeding or the subtle neurologic change that needs immediate attention, and the ECMO patient is monitored more intensively than almost any other patient in the unit precisely because the margin for missed complications is small.
The pharmacist manages the anticoagulation strategy, which is the central pharmacologic challenge of ECMO and the determinant of the bleeding-versus-thrombosis balance that EOLIA’s safety profile turned on. The pharmacist also manages sedation, analgesia, and the altered drug pharmacokinetics that the circuit introduces, since the membrane and tubing can sequester certain drugs and change their effective dosing. The pharmacist who tailors anticoagulation conservatively, as the EOLIA centers did, contributes directly to the safety profile.
The APP carries the protocol and the continuity across shifts and days. ECMO runs for a median of around 8 to 10 days, and the consistency of the lung-rest strategy, the anticoagulation targets, the weaning plan, and the daily assessment across that span depends on documentation and handoff that the APP often anchors. The APP who keeps the strategy coherent across a long ECMO run prevents the drift that undermines a careful plan.
This is interprofessional medicine at its most concentrated. No single discipline can run ECMO. The therapy exists only as a coordinated team performance, and the evidence suggests the quality of that performance matters as much as the decision to use the therapy at all.
ECMO reliably rests the lung. Whether resting the lung this way saves more lives is a question the field is still answering, and saying so out loud is what credibility requires.
Bedside / Workplace Takeaways
Frame ECMO honestly with families and teams. The defensible statement is that VV-ECMO is a reasonable, guideline-endorsed option for selected very severe ARDS at experienced centers, with probable but not definitively proven mortality benefit. Avoid presenting it as a therapy with a settled survival advantage, because EOLIA did not show that.
Refer early rather than late when ECMO is being considered. The most defensible reading of EOLIA is that early ECMO, before multi-organ failure accrues, is the strategy with the best case for benefit. The 28% crossover in the control group occurred at a mean of 6.5 days in patients who were deteriorating, which argues for earlier rather than later referral to an ECMO center.
Optimize conventional therapy first. ECMO is escalation after evidence-based conventional management, which includes lung-protective ventilation, prone positioning, and neuromuscular blockade in the most severe cases. A patient who has not had an adequate trial of prone positioning is generally not yet an ECMO patient.
Once on ECMO, target lung rest with attention to driving pressure. The observational evidence points to driving pressure during the first days on ECMO as the ventilator variable most associated with survival. Keep driving pressure low. Survivors in the pooled data had a mean driving pressure around 17 cm H2O.
Do not chase the lowest possible tidal volume. REST tested ultra-low tidal volume facilitated by carbon dioxide removal and found no mortality benefit and a higher rate of serious adverse events including intracranial hemorrhage. Ultraprotective settings are reasonable, but pushing toward 3 mL/kg with extracorporeal support is not supported by outcome data and carries real harm.
Titrate carbon dioxide removal gradually after cannulation. Rapid correction of hypercapnia after ECMO initiation has been associated with neurologic complications. The perfusionist and intensivist should lower carbon dioxide in a controlled way rather than maximally.
Manage anticoagulation conservatively. EOLIA’s favorable neurologic safety profile was attributed partly to careful, low-intensity anticoagulation. The pharmacist and team should aim for the anticoagulation strategy that balances thrombosis against bleeding rather than defaulting to aggressive targets.
Treat ECMO as a team performance, not a device. The outcome depends on the perfusionist, intensivist, RT, nurse, pharmacist, and APP working in coordination. Centers with experience and explicit protocols achieve better safety than centers using ECMO occasionally, which is why guidelines specify experienced centers.
Teaching Pearl
The next time you watch a patient stabilize on ECMO, the saturation recovering and the ventilator coming down, hold two thoughts at the same time. The first is that you have genuinely reduced the mechanical forces injuring this patient’s lung, which is a real and worthwhile thing. The second is that whether this intervention will improve this patient’s survival, beyond what careful conventional care plus rescue ECMO would have achieved, is a question the evidence answers with probability rather than certainty. The visible improvement in front of you is real. It is not the same as proof of mortality benefit. A clinician who can hold both thoughts is a clinician who will use ECMO well, refer for it at the right time, ventilate the rested lung sensibly, and describe it honestly to the family.
Teach your fellows, your new respiratory therapists, your perfusionists, your nurses, and your APPs the difference between resting the lung and saving the life. The first is mechanical and demonstrable. The second is probable, contested, and dependent on the team. Conflating them is how enthusiasm outruns evidence, and severe ARDS is a place where that gap can hurt people.
What We Should Not Over-Assume
This article is built around not over-assuming, so this section is the center of it rather than an afterthought.
We should not assume EOLIA proved ECMO works. It did not meet its primary endpoint. The case for benefit rests on a Bayesian reanalysis whose conclusion depends on the prior, and on meta-analyses built from two trials, one of which has well-known methodological limitations. Reasonable experts read this evidence differently, and a clinician who tells a family that ECMO is proven to improve survival in severe ARDS is overstating what the trials show.
We should not assume more lung rest is better lung protection. REST tested that proposition directly, pushing tidal volume toward 3 mL/kg with carbon dioxide removal, and found no mortality benefit and a higher rate of serious adverse events. The physiologic appeal of ever-lower tidal volume is not matched by outcome evidence at the extreme.
We should not assume the driving pressure association is a proven causal target. Serpa Neto’s data are observational. Lower driving pressure on ECMO is associated with survival, which is a reason to attend to it, but the association could partly reflect that sicker lungs both have higher driving pressure and worse outcomes. A randomized trial of a driving-pressure-targeted strategy on ECMO has not been done.
We should not assume the EOLIA safety profile generalizes to every center. The low rate of hemorrhagic complications was achieved in experienced centers with careful anticoagulation. A center new to ECMO, or one using it occasionally, should not assume it will replicate those safety numbers, which is exactly why guidelines specify experienced centers.
And we should not assume ECMO is the answer when conventional therapy has not been optimized. The patient who has not had adequate prone positioning, neuromuscular blockade in the severe case, or a genuine lung-protective strategy has options that come before ECMO. ECMO is escalation, not substitution.
Limitations
The evidence base for VV-ECMO in ARDS rests on a small number of randomized trials. EOLIA and CESAR are the only two modern RCTs, and they enrolled different populations under different protocols across a decade of evolving practice. The meta-analyses that find benefit are pooling these two trials, and the strength of a meta-analysis is bounded by the trials inside it. The Bayesian reanalysis is a reinterpretation rather than new data. The ventilation-strategy evidence on ECMO is largely observational, with the single large RCT of extreme ultraprotective ventilation, REST, being negative. There is no large multicenter RCT establishing the optimal ventilator settings during ECMO, and most practice is guided by expert opinion and association data. The populations studied are very severe ARDS at experienced centers, which limits generalization to less severe patients, less experienced centers, and health systems without rapid ECMO access. This is a field where the physiology is well understood and the outcome evidence is genuinely incomplete, and the honest clinician holds both.
Bottom Line
VV-ECMO reliably rests the lung. It reduces the tidal volume, plateau pressure, and driving pressure applied to an injured lung while maintaining gas exchange, and that mechanical effect is well-documented. Whether resting the lung this way improves survival is the harder question, and the honest answer is that the benefit is probable in selected very severe ARDS at experienced centers and still genuinely debated, because the one dedicated RCT did not meet its primary endpoint and the strategy of maximal lung rest through ultra-low tidal volume failed in a separate trial. The driving pressure association is the most actionable bedside signal once ECMO is running, held as an association rather than a proven target. The team running ECMO matters as much as the decision to use it. A publication that charges for clinical intelligence owes its readers this version, the one that distinguishes what ECMO demonstrably does from what we hope it does, rather than the simpler and more confident story that the evidence does not support.
Javier Amador-Castaneda, BHS, RRT, FCCM | Founder & CEO, ICCN
Reference
Combes A, Hajage D, Capellier G, et al; EOLIA Trial Group, REVA, and ECMONet. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378(21):1965-1975. doi:10.1056/NEJMoa1800385
Goligher EC, Tomlinson G, Hajage D, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome and posterior probability of mortality benefit in a post hoc Bayesian analysis of a randomized clinical trial. JAMA. 2018;320(21):2251-2259. doi:10.1001/jama.2018.14276
Munshi L, Walkey A, Goligher E, Pham T, Uleryk EM, Fan E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: a systematic review and meta-analysis. Lancet Respir Med. 2019;7(2):163-172. doi:10.1016/S2213-2600(18)30452-1
Combes A, Peek GJ, Hajage D, et al. ECMO for severe ARDS: systematic review and individual patient data meta-analysis. Intensive Care Med. 2020;46(11):2048-2057. doi:10.1007/s00134-020-06248-3
Peek GJ, Mugford M, Tiruvoipati R, et al; CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374(9698):1351-1363. doi:10.1016/S0140-6736(09)61069-2
Combes A, Fanelli V, Pham T, Ranieri VM; European Society of Intensive Care Medicine Trials Group and the SUPERNOVA investigators. Feasibility and safety of extracorporeal CO2 removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive Care Med. 2019;45(5):592-600. doi:10.1007/s00134-019-05567-4
McNamee JJ, Gillies MA, Barrett NA, et al; REST Investigators. Effect of lower tidal volume ventilation facilitated by extracorporeal carbon dioxide removal vs standard care ventilation on 90-day mortality in patients with acute hypoxemic respiratory failure: the REST randomized clinical trial. JAMA. 2021;326(11):1013-1023. doi:10.1001/jama.2021.13374
Bein T, Weber-Carstens S, Goldmann A, et al. Lower tidal volume strategy (≈3 mL/kg) combined with extracorporeal CO2 removal versus conventional protective ventilation (6 mL/kg) in severe ARDS: the prospective randomized Xtravent-study. Intensive Care Med. 2013;39(5):847-856. doi:10.1007/s00134-013-2787-1
Serpa Neto A, Schmidt M, Azevedo LCP, et al; ReVA Research Network and the PROVE Network Investigators. Associations between ventilator settings during extracorporeal membrane oxygenation for refractory hypoxemia and outcome in patients with acute respiratory distress syndrome: a pooled individual patient data analysis. Intensive Care Med. 2016;42(11):1672-1684. doi:10.1007/s00134-016-4507-0
Schmidt M, Pham T, Arcadipane A, et al; International ECMO Network (ECMONet) and the LIFEGARDS Study Group. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: an international multicenter prospective cohort. Am J Respir Crit Care Med. 2019;200(8):1002-1012. doi:10.1164/rccm.201806-1094OC
Amato MBP, Meade MO, Slutsky AS, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747-755. doi:10.1056/NEJMsa1410639
Del Sorbo L, Goffi A, Tomlinson G, et al. Effect of driving pressure change during extracorporeal membrane oxygenation in adults with acute respiratory distress syndrome: a randomized crossover physiologic study. Crit Care Med. 2020;48(12):1771-1778. doi:10.1097/CCM.0000000000004637
Abrams D, Schmidt M, Pham T, et al. Mechanical ventilation for acute respiratory distress syndrome during extracorporeal life support: research and practice. Am J Respir Crit Care Med. 2020;201(5):514-525. doi:10.1164/rccm.201907-1283CI
Guervilly C, Fournier T, Chommeloux J, et al. Ultra-lung-protective ventilation and biotrauma in severe ARDS patients on veno-venous extracorporeal membrane oxygenation: a randomized controlled study. Crit Care. 2022;26(1):383. doi:10.1186/s13054-022-04272-x
Quintel M, Bartlett RH, Grocott MPW, et al. Extracorporeal membrane oxygenation for respiratory failure. Anesthesiology. 2020;132(5):1257-1276. doi:10.1097/ALN.0000000000003221
Clinical Disclaimer
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.