

The Pressure Behind the Pressure
What Esophageal Manometry and Transpulmonary Pressure Mean for the 2026 ICU

The number on the ventilator screen reports the pressure the machine is delivering. The pressure the lung actually experiences is transpulmonary pressure, which lives inside the chest and requires an esophageal balloon to measure. For most of the last forty years we have lived with that gap. We have built every lung protection strategy on airway pressure proxies (plateau pressure, driving pressure, mechanical power) and counted on the chest wall and the patient to behave like the assumptions in the equation. That works in average chest wall mechanics. It breaks in everyone else. Esophageal manometry has been the answer to that breakdown for almost two decades, and a 2026 Medical Gas Research paper by Schultz makes the case that the tool deserves a place at every modern ICU bedside.¹
Why This Matters
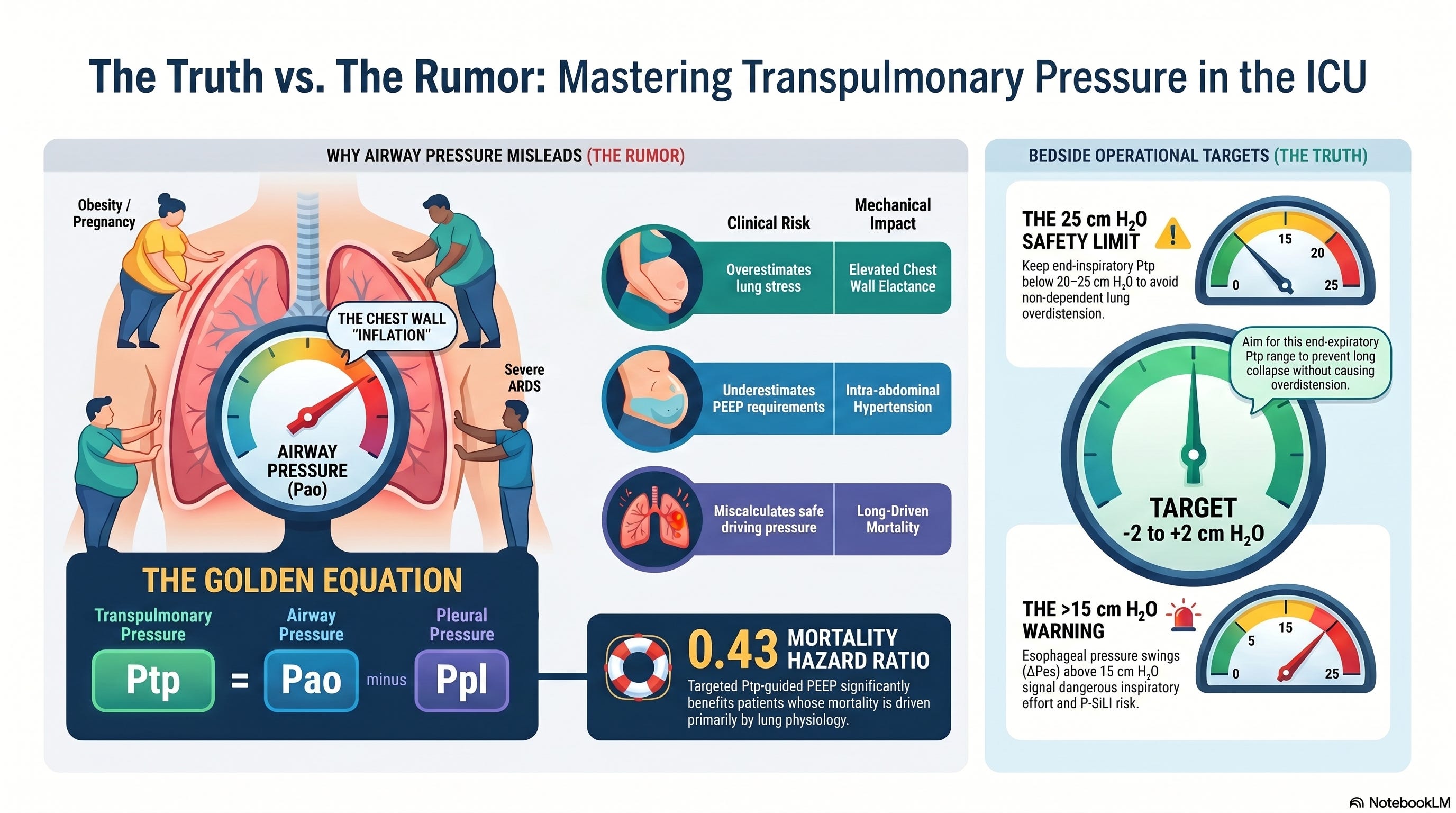
The lungs do not feel airway pressure. They feel transpulmonary pressure, which is airway pressure minus pleural pressure.²⁻⁷ Two patients with the same plateau pressure can have radically different lung stress depending on what their chest wall and abdomen are doing. The obese patient. The patient with intra-abdominal hypertension. The pancreatitis patient with massive third-space loss. The post-surgical patient with abdominal binders and drains. The ARDS patient who is breathing spontaneously. In each of these patients, airway pressure tells a story the lung is not living. Esophageal manometry, used as a surrogate for pleural pressure, lets you do the subtraction and see the actual pressure the lung experiences.
The last two Tuesday articles laid the foundation for this one. Two weeks ago I wrote about P-SILI and made the case that effort is a vital sign. Last week I wrote about post-extubation respiratory support and made the case that risk stratification before extubation is what prevents reintubation. Esophageal manometry is the tool that operationalizes both. Drive-aware care is impossible without a way to measure pleural pressure swings. Personalized PEEP, lung-protective ventilation in obese or ARDS patients, and the safe titration of ultraprotective ventilation on ECMO or extracorporeal CO₂ removal all run through transpulmonary pressure as the unifying variable.¹ ² ⁶
For the interprofessional ICU team this is the operational instrument that converts our theoretical conversations about lung stress into bedside numbers we can act on. The RT places the catheter and reads the waveform. The intensivist titrates PEEP against the measured signal. The nurse identifies the patient who is becoming dyssynchronous. The pharmacist tunes sedation to the swing. The APP carries the plan across shifts. The perfusionist enters when transpulmonary pressure says the lung is not protectable on the ventilator alone.
The Study / Evidence in Context
The anchor for this article is the April 2026 Medical Gas Research paper by Schultz on esophageal pressure monitoring as the bridge to ultraprotective ventilation under ECCO2R.¹ The paper synthesizes the technical concepts of pleural pressure surrogacy, transpulmonary pressure calculation, the elastance-derived and direct methods, and the ultraprotective ventilation strategy (tidal volume below 4 mL/kg, plateau pressure below 25 cm H₂O) that an esophageal-pressure-guided approach makes safe in patients who cannot be ventilated within those limits without extracorporeal support. Its takeaway is that transpulmonary pressure is the variable that connects every other modern conversation about lung protection (driving pressure, mechanical power, P-SILI, ECMO escalation) into a coherent strategy.
To read that synthesis correctly, the team needs the historical scaffolding underneath it.
The 2008 EPVent trial by Talmor and colleagues was the first randomized signal.³ Sixty-one patients with acute lung injury were randomized to esophageal-pressure-guided PEEP titration (targeting a positive end-expiratory transpulmonary pressure) versus the ARDSnet PEEP/FiO₂ table. The PaO₂/FiO₂ ratio at 72 hours was significantly better in the esophageal-pressure-guided group, respiratory system compliance was better, and a mortality signal favored the intervention, although the trial was underpowered to confirm it. The paper changed how the academic ARDS community thought about PEEP titration.
The 2019 EPVent-2 trial by Beitler and colleagues was the larger confirmatory test.⁴ Two hundred patients with moderate to severe ARDS were randomized to esophageal-pressure-guided PEEP versus an empirical high PEEP/FiO₂ strategy. The primary composite outcome (death and ventilator-free days through day 28) showed no significant difference between the groups. The trial was widely read as a setback for esophageal manometry as a routine ICU tool, and many programs that had built esophageal pressure workflows in the wake of EPVent walked them back.
The 2021 EPVent-2 reanalysis by Sarge and colleagues complicated that reading.⁵ A risk-based, mechanistic post-hoc analysis showed that the intervention’s effect depended on baseline multi-organ dysfunction. Patients with lower APACHE-II scores benefited from esophageal-pressure-guided PEEP, with a 60-day mortality hazard ratio of 0.43 (95% CI 0.20 to 0.92), while patients with higher APACHE-II scores did not. The interpretation is that esophageal-pressure-guided PEEP is a lung-protective strategy and not a multi-organ-failure rescue strategy. In patients whose mortality is driven primarily by lung physiology rather than by septic shock or multi-organ collapse, the technique appears to help.
The 2024 narrative review by Ball, Talmor, and Pelosi in Critical Care covers the technical and clinical landscape comprehensively.² The authors make a careful pros-and-cons case for esophageal manometry, noting that the technique remains underused despite consistent physiologic evidence supporting its use. The pros include the ability to partition respiratory mechanics between lung and chest wall, to identify lung recruitment versus chest wall recruitment in response to PEEP, to quantify inspiratory effort during assisted ventilation, and to guide safe transgression of conventional airway pressure limits when chest wall elastance is elevated. The cons include the technical learning curve, balloon position and filling uncertainties, the heterogeneity of how pleural pressure is distributed along the vertical gradient of the lung, and the absence of a definitive RCT confirming a mortality benefit from a transpulmonary-pressure-guided strategy.
The 2024 Mauri crossover trial in Intensive Care Medicine added an important bedside-relevant data point.⁶ The investigators randomized intubated ARDS patients on pressure support ventilation to personalized PEEP set by simultaneous electrical impedance tomography and transpulmonary driving pressure monitoring versus a conventional lower PEEP/FiO₂ table. Personalized PEEP based on the combined approach produced more homogeneous regional ventilation, lower driving transpulmonary pressure, and lower inspiratory effort. This is exactly the type of trial that the field had needed: a study asking whether transpulmonary pressure improves the upstream physiology that lung-protective ventilation is built on, rather than asking whether it improves mortality across heterogeneous populations.
The 2025 Zhao trial in World Journal of Surgery extended the signal into a specific high-risk population: ARDS associated with severe acute pancreatitis.¹⁵ The intra-abdominal hypertension and elevated chest wall elastance in this population make airway-pressure-based PEEP titration particularly unreliable. Patients randomized to esophageal-pressure-guided ventilation had lower plateau pressure, lower driving pressure, and better compliance at 72 hours compared with conventional titration. This is the population in which the technique was always going to have the strongest signal, and the trial confirms what the physiology predicted.
The 2014 PLUG group consensus by Akoumianaki and colleagues remains the methodological reference for how to do this at the bedside.⁸ The 2016 Mauri ICM review and the 2018 Yoshida AJRCCM study on regional pleural pressure distribution remain the conceptual references for the limits of esophageal pressure as a surrogate for the dependent lung.⁷ ⁹ The 2021 Baedorf Kassis and Talmor “how I do it” paper in Critical Care remains the most readable practical guide to building an esophageal manometry workflow in a unit that does not yet have one.¹⁰
What Stood Out
A few things from the 2026 Schultz synthesis and the supporting literature should reorganize how the interprofessional team thinks about esophageal manometry in practice.
First, transpulmonary pressure is the unifying variable in modern lung protection. Driving pressure, mechanical power, the PEEP titration debate, P-SILI, and ultraprotective ventilation on ECCO2R or ECMO all converge on transpulmonary pressure as the actual stress variable.¹ ² ⁷ The team that treats transpulmonary pressure as primary and airway pressure as a proxy is the team that can hold all of these conversations consistently. The team that treats airway pressure as primary is the team that ends up with five different protocols for five different physiologic problems.
Second, the elastance-derived method estimates end-inspiratory lung stress without requiring direct esophageal pressure measurement. When you do not have a balloon in place, you can estimate transpulmonary pressure at end-inspiration by multiplying plateau pressure by the ratio of lung elastance to total respiratory system elastance. A value below 20 to 25 cm H₂O is widely considered the upper safety limit during passive ventilation.² ⁷ ⁹ The technique is approximate but useful, and it can serve as a screening method to identify which patients deserve a balloon catheter.
Third, the end-expiratory transpulmonary pressure target is widely accepted in the literature. A target of zero to slightly positive end-expiratory transpulmonary pressure prevents end-expiratory collapse without producing dangerous overdistension.¹ ² ¹⁰ The PEEP needed to reach this target is highly variable. A thin elderly patient may reach it at PEEP 8. An obese patient or one with intra-abdominal hypertension may need PEEP 18 or higher. Airway-pressure-based PEEP titration tables miss this heterogeneity by design.
Fourth, the inspiratory effort signal is the most clinically actionable piece of the technique in the assisted-ventilation era. Esophageal pressure swing (ΔPes) during inspiration is the bedside reference standard for inspiratory effort.² ¹⁰ ¹¹ A swing under 10 cm H₂O is generally compatible with lung-protective effort. A swing above 15 cm H₂O is a warning sign. Above 20 cm H₂O is a call to action. This is exactly the signal that operationalizes the P-SILI prevention strategy we covered two weeks ago.
Fifth, the technique works in the populations where airway pressure most predictably misleads. Obesity, intra-abdominal hypertension, pregnancy, post-abdominal surgery, ascites, large pleural effusions, and chest wall edema all elevate chest wall elastance and inflate airway pressure without inflating the lung. In every one of these populations, airway-pressure-based ventilation underestimates the PEEP the lung needs and overestimates the plateau pressure that is “safe.” Esophageal manometry reveals what airway pressure cannot.¹ ² ¹⁵
Two patients with the same plateau pressure can have radically different lung stress. The tool that tells you which is which has been at the bedside for fifteen years, and we still do not use it consistently.
Physiologic, Clinical, Leadership, or Ethical Interpretation
Here is my read.
The EPVent-2 trial did not kill esophageal manometry. It revealed what the technique can and cannot do. A randomized trial of any single ventilator intervention in moderate-to-severe ARDS is a trial against a heterogeneous population in which mortality is driven by everything from septic shock to multi-organ failure to renal replacement burden. Expecting one PEEP-titration strategy to move all-cause mortality in that population is asking the technique to do work it was not designed to do. The 2021 reanalysis made the actual finding clear. In patients whose dying is driven by lung physiology rather than by extra-pulmonary collapse, esophageal-pressure-guided PEEP appears to help. In patients whose dying is driven by something else, it does not.⁵
This is the same kind of result the field has reported for years with other lung-protective interventions. The benefit is real, and it lives in the right phenotype. Identifying the phenotype is part of the work.
For the interprofessional team this maps onto a workflow that should look familiar by now.
The respiratory therapist is the central operator of esophageal manometry. RT teams that have built this competency can place the catheter, validate the position with an occlusion test, set the appropriate balloon filling volume, and read the waveform with confidence.⁸ ¹⁰ ¹³ The catheter is technically simple and competence is teachable, which means the limiting factor is institutional commitment to training. RTs who own esophageal manometry give the rest of the team a number to act on. RTs who do not are stuck reading airway pressure surrogates and hoping the assumptions hold.
The intensivist uses the transpulmonary pressure signal to titrate PEEP, set plateau pressure limits, identify the patient who is failing conventional ventilation because of chest wall mechanics rather than lung disease, and decide when to escalate to ECMO or extracorporeal CO₂ removal. The decision to escalate to extracorporeal support is much cleaner when the team knows the transpulmonary driving pressure is above 12 cm H₂O at the lowest tidal volume the patient tolerates. Without the number, escalation is a clinical gestalt.¹ ¹⁵
The nurse is the bedside discipline most likely to notice the patient’s tolerance of the catheter, the patient who is dyssynchronous with the ventilator, the patient whose esophageal pressure swing on the monitor is rising as their respiratory rate climbs. A drive-aware nurse who can read the esophageal pressure tracing is doing P-SILI prevention work in real time.
The pharmacist tunes sedation to the esophageal pressure signal. The patient with a high inspiratory effort despite optimal ventilator settings may need additional sedation, an opioid, or neuromuscular blockade. The pharmacist who is in the room as part of the daily ventilator review is the discipline that integrates the drug strategy with the physiologic signal.
The APP maintains the protocol and the handoff. Esophageal manometry workflows that drift across shifts produce inconsistent numbers, and inconsistent numbers do not get acted on. The APP who walks the bedside, checks the balloon position, confirms the calibration, and documents the day’s targets is the discipline that keeps the technique alive in a unit that adopts it.
The perfusionist enters when transpulmonary pressure says the lung cannot be protected by conventional ventilation. A driving transpulmonary pressure above 12 cm H₂O at the lowest tolerable tidal volume, or a plateau transpulmonary pressure above 20 to 25 cm H₂O at standard settings, is a strong indicator that the patient needs an extracorporeal CO₂ removal or VV ECMO consultation.¹ The team that consults perfusion based on transpulmonary pressure rather than airway pressure makes the call earlier and more accurately.
This is the natural interprofessional architecture for a tool that requires multiple disciplines to operate well. The unit that builds it once gets a workflow that pays off in every ARDS patient, every obese patient, every patient with intra-abdominal hypertension, every patient on ECCO2R or ECMO, and every patient on assisted ventilation with a question about drive.
Bedside / Workplace Takeaways
Place the catheter early when you are going to use it. The right time to insert an esophageal balloon catheter is when the patient is intubated, sedated, and you anticipate complex respiratory mechanics. Inserting it on day three after airway pressure has already gone wrong is a missed opportunity.
Validate the position with an occlusion test. Perform an end-expiratory or end-inspiratory occlusion and confirm that ΔPes / ΔPaw is between 0.8 and 1.2.⁸ ¹³ A ratio outside that range means the catheter is either too proximal, too distal, or the balloon volume is wrong. Do not interpret pressures until the occlusion test passes.
Set the right balloon filling volume. Most adult balloons require 1 to 4 mL of air depending on the manufacturer and the patient’s chest wall mechanics. Underfilling produces falsely low pressures. Overfilling produces falsely high pressures.¹⁰ ¹³ Confirm the volume on insertion and recheck if the tracing looks wrong.
Target end-expiratory transpulmonary pressure between minus 2 and plus 2 cm H₂O. This is the widely accepted PEEP titration target in ARDS.¹ ² ¹⁰ A value clearly negative at end-expiration means the dependent lung is collapsing and the patient needs more PEEP. A value strongly positive means you are overdistending and PEEP can come down.
Keep end-inspiratory transpulmonary pressure below 20 to 25 cm H₂O during passive ventilation. This is the consensus upper safety limit.² ⁷ ⁹ Above this threshold the non-dependent lung is at risk of overdistension regardless of what the plateau pressure number says.
Read esophageal pressure swing during assisted ventilation as the inspiratory effort signal. A swing under 10 cm H₂O is generally lung-protective effort. Above 15 cm H₂O is a warning. Above 20 cm H₂O is a call to action.² ¹⁰ ¹¹
Use the elastance-derived method when you do not have a balloon. Multiply plateau pressure by the ratio of lung elastance to total respiratory system elastance to estimate end-inspiratory transpulmonary pressure. This screening method can identify the patient who deserves a balloon.
Reach for the catheter in obesity, intra-abdominal hypertension, and pancreatitis. These are the phenotypes where airway pressure most predictably misleads.¹⁵ A balloon catheter in these patients regularly changes ventilator settings within the first hour.
Use the signal to time the escalation conversation with the perfusion team. Driving transpulmonary pressure above 12 cm H₂O at the lowest tolerable tidal volume, or plateau transpulmonary pressure consistently above 20 to 25 cm H₂O, is a stronger trigger for ECCO2R or VV ECMO consultation than airway pressure thresholds alone.¹
Build a protocol with explicit numbers. Targets without numbers do not get acted on across shifts. Document the end-expiratory transpulmonary pressure target, the end-inspiratory transpulmonary pressure limit, the esophageal pressure swing thresholds, and the calibration timing in the order set.
Listen to the following podcast:
Teaching Pearl
The next time you see a high plateau pressure in an obese or ARDS patient and reach for the “decrease tidal volume” reflex, pause. Ask yourself a single question. Is this airway pressure telling me about the lung, or about the chest wall. The answer is sitting in the esophagus, two centimeters above the gastroesophageal junction, waiting for someone to put a catheter there and read it. The patient whose chest wall is doing the work is the patient whose lung is being underventilated and whose PEEP is too low. Lowering the tidal volume in that patient makes the underventilation worse and does not protect a lung that was never being stressed in the first place. The patient whose lung is doing the work is the patient whose tidal volume is genuinely too high. Without the esophageal pressure measurement, both patients look identical on your ventilator screen. The balloon catheter is what gives you a way to tell them apart.
Teach your fellows, your new RTs, your nurses, your APPs the transpulmonary pressure as the truth and the airway pressure as the rumor. The team that reads both is the team that protects the lung that needs protecting and respects the chest wall that does not.
What We Should Not Over-Assume
EPVent-2 is not a license to abandon esophageal manometry. The trial measured a primary outcome of all-cause mortality and ventilator-free days in a heterogeneous moderate-to-severe ARDS population and showed no difference, which is the result the field should have expected when a single ventilator intervention is tested against all-cause mortality in a population with multiple competing risks.⁴ The 2021 reanalysis showed that in the phenotype where lung physiology drives mortality, the technique works.⁵ The 2024 Mauri RCT in assisted-ventilation patients showed that the technique improves the upstream physiology of lung-protective ventilation.⁶ The 2025 Zhao RCT in pancreatitis-associated ARDS showed that the technique improves mechanics where airway pressure most predictably misleads.¹⁵ The case for routine availability in every ICU is at least as strong as the case for routine bronchoscopy or routine echocardiography, both of which sit at the bedside without a mortality RCT to justify them.
We also should not assume that esophageal pressure equals the average pleural pressure across the lung. It does not. Esophageal pressure tracks regional pleural pressure in the mid-dependent zone, and the vertical gradient of pleural pressure in ARDS means the dependent lung sees a higher pleural pressure and the non-dependent lung sees a lower one.⁷ ⁹ A clinician who treats esophageal pressure as a perfect average will overestimate lung protection in the dependent zone and underestimate non-dependent overdistension. The right read is that esophageal pressure is a useful surrogate rather than a perfect one, and the elastance-derived estimate is a complement rather than a substitute.
Finally, we should not assume the technique is harder than the bedside experience suggests. RTs and intensivists who have placed a few catheters and run a few occlusion tests find the technique technically simple. The barriers are institutional commitment, training, and the will to make the technique a routine option rather than a niche tool.
Limitations
The 2026 Schultz synthesis is a narrative review and a conceptual framework rather than a systematic evidence base.¹ The EPVent-2 reanalysis is post-hoc and exploratory, with the usual cautions that apply to any post-hoc finding.⁵ The 2024 Mauri trial is a single-center crossover study of physiologic endpoints, not a multicenter mortality trial.⁶ The 2025 Zhao trial is a single-center study in a specific population, with intermediate outcome targets rather than mortality.¹⁵ The technique itself depends on operator skill, balloon position, balloon volume, and patient body habitus, all of which introduce measurement variability that is hard to eliminate.²
The field also still lacks the multicenter trial that the proponents have been calling for since EPVent-2: a randomized trial in a phenotype-restricted population (low APACHE-II, lung-driven mortality) comparing esophageal-pressure-guided ventilation against contemporary care with mortality as the primary outcome. Until that trial exists, the evidence base sits at the level of physiology and intermediate outcomes, and the routine use of the technique remains a clinical commitment rather than a guideline mandate.
Bottom Line
The pressure on your screen reflects what the ventilator is doing. The lung itself feels transpulmonary pressure, and esophageal manometry is the bedside tool that closes the gap between the two. The 2024 to 2026 evidence has refined our understanding of where the technique helps most: lung-driven mortality phenotypes, obesity, intra-abdominal hypertension, pancreatitis, assisted ventilation with drive concerns, and ultraprotective ventilation on extracorporeal support. The ICU that builds the workflow once gets a tool that pays off across every complex ventilator decision. The ICU that does not is reading the rumor and acting on it as if it were the truth.
Javier Amador-Castaneda, BHS, RRT, FCCM | Founder & CEO, ICCN
Reference
Schultz MJ. Esophageal pressure monitoring and ECCO2R: a personalized approach to ultraprotective mechanical ventilation in ARDS patients. Med Gas Res. 2026. doi:10.4103/mgr.MEDGASRES-D-25-00049
Ball L, Talmor D, Pelosi P. Transpulmonary pressure monitoring in critically ill patients: pros and cons. Crit Care. 2024;28(1):177. doi:10.1186/s13054-024-04950-y
Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation guided by esophageal pressure in acute lung injury. N Engl J Med. 2008;359(20):2095-2104. doi:10.1056/NEJMoa0708638
Beitler JR, Sarge T, Banner-Goodspeed VM, et al; EPVent-2 Study Group. Effect of titrating positive end-expiratory pressure (PEEP) with an esophageal pressure-guided strategy vs an empirical high PEEP-FIO2 strategy on death and days free from mechanical ventilation among patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA. 2019;321(9):846-857. doi:10.1001/jama.2019.0555
Sarge T, Baedorf-Kassis E, Banner-Goodspeed V, et al. Effect of esophageal pressure-guided positive end-expiratory pressure on survival from acute respiratory distress syndrome: a risk-based and mechanistic reanalysis of the EPVent-2 trial. Am J Respir Crit Care Med. 2021;204(10):1153-1163. doi:10.1164/rccm.202009-3539OC
Mauri T, Grieco DL, Spinelli E, et al. Personalized positive end-expiratory pressure in spontaneously breathing patients with acute respiratory distress syndrome by simultaneous electrical impedance tomography and transpulmonary pressure monitoring: a randomized crossover trial. Intensive Care Med. 2024;50(12):2125-2137. doi:10.1007/s00134-024-07695-y
Mauri T, Yoshida T, Bellani G, et al. Esophageal and transpulmonary pressure in the clinical setting: meaning, usefulness and perspectives. Intensive Care Med. 2016;42(9):1360-1373. doi:10.1007/s00134-016-4400-x
Akoumianaki E, Maggiore SM, Valenza F, et al. The application of esophageal pressure measurement in patients with respiratory failure. Am J Respir Crit Care Med. 2014;189(5):520-531. doi:10.1164/rccm.201312-2193CI
Yoshida T, Amato MBP, Grieco DL, et al. Esophageal manometry and regional transpulmonary pressure in lung injury. Am J Respir Crit Care Med. 2018;197(8):1018-1026. doi:10.1164/rccm.201709-1806OC
Baedorf Kassis E, Talmor D. Clinical application of esophageal manometry: how I do it. Crit Care. 2021;25(1):6. doi:10.1186/s13054-020-03453-w
Shimatani T, Kyogoku M, Ito Y, Takeuchi M, Khemani RG. Fundamental concepts and the latest evidence for esophageal pressure monitoring. J Intensive Care. 2023;11(1):22. doi:10.1186/s40560-023-00671-6
Somhorst P, Mousa A, Jonkman AH. Setting positive end-expiratory pressure: the use of esophageal pressure measurements. Curr Opin Crit Care. 2024;30(1):44-52. doi:10.1097/MCC.0000000000001120
Mojoli F, Torriglia F, Orlando A, Bianchi I, Arisi E, Pozzi M. Technical aspects of bedside respiratory monitoring of transpulmonary pressure. Ann Transl Med. 2018;6(19):377. doi:10.21037/atm.2018.08.37
Spinelli E, Scaramuzzo G, Slobod D, Mauri T. Understanding cardiopulmonary interactions through esophageal pressure monitoring. Front Physiol. 2023;14:1221829. doi:10.3389/fphys.2023.1221829
Zhao Y, Zhang S, Liu C, Wang X. Individualized lung-protective ventilation strategy based on esophageal pressure monitoring in patients with ARDS associated with severe acute pancreatitis: a randomized controlled trial. World J Surg. 2025. doi:10.1002/wjs.12676
Clinical Disclaimer
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.