

Two Documents. Same Year. Opposite Verdicts. The Dex Versus Propofol Reckoning Your Unit Has Been Putting Off
What 1,404 patients across 41 UK ICUs, a refreshed SCCM guideline, and twenty years of sedation trials actually tell us. And why the question your team keeps asking is the wrong question.

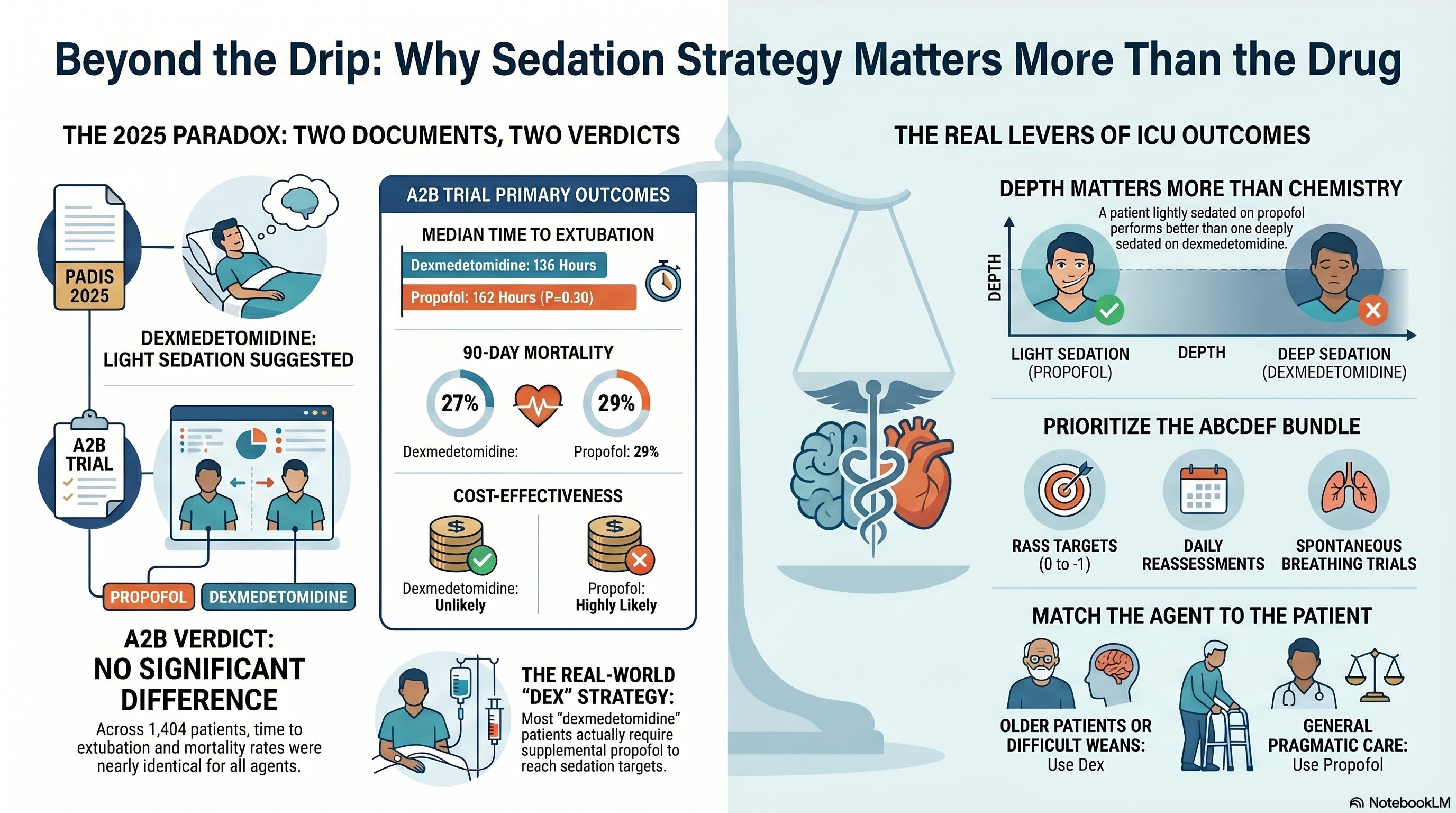
In March 2025, the Society of Critical Care Medicine released a focused update to the PADIS guidelines and made a conditional recommendation that ICU teams use dexmedetomidine over propofol when light sedation or delirium reduction are the priorities.
Ten weeks later, JAMA published the A2B trial. One thousand four hundred and four patients. Forty-one UK intensive care units. Three arms (dexmedetomidine, clonidine, propofol). The verdict from the lead investigator was, in his own words, that he would continue to use propofol as a first-line drug.
Two carefully developed, well-funded, widely cited 2025 documents about the same question. Opposite verdicts. Same year.
This is what the bedside has been asked to live with for the past twelve months. And it is the reason your sedation rounds feel less settled than they did in 2024.
Why This Matters
Sedation is not a side issue in the ICU. It is one of the three or four highest-leverage decisions on your unit on any given day. It governs ventilator time. It governs delirium incidence. It governs the trajectory of ICU-acquired weakness. It governs how families experience the unit. It governs cost.
The PADIS focused update and the A2B trial do not disagree on whether sedation matters. They disagree on whether the choice of agent is the right place to spend your unit’s optimization energy.
If you are an intensivist writing the order, an RT running a spontaneous breathing trial, a nurse titrating the drip, an APP managing the trajectory, a pharmacist stewarding the formulary, or a perfusionist handing off from bypass, this controversy lands on you. You cannot opt out by waiting for the next guideline. The next guideline will arrive into the same evidence base.
ICCN’s read on the controversy: both documents are correct in their own domains, and both are answering a narrower question than the one the field actually needs to answer.
The new ICCN website is open. Two features are worth a look. The Research section organizes our coverage of the trials and reviews driving practice change, by system and continuously updated from 26 different journals. The Article section holds the full ICCN back catalog, searchable and free to browse. Both are built to the same standard as the Substack you are reading. Explore ICCN.
The Study and the Evidence in Context
A2B: The largest head-to-head sedation trial in a decade
A2B was a pragmatic, open-label, multicentre randomised trial conducted across 41 ICUs in the United Kingdom. The investigators enrolled critically ill adults expected to need at least 48 hours of mechanical ventilation and randomised them to one of three primary sedation strategies: dexmedetomidine-based, clonidine-based, or propofol-based. Supplemental propofol was permitted when needed. The primary outcome was time from randomisation to successful extubation. Secondary outcomes included mortality at ICU discharge, 90 days, and 180 days, sedation quality, delirium rates, and cardiovascular adverse events.
Of the 1,404 patients in the analysis population, the mean age was 59.2 years (SD 14.9), 64 percent were male, and the mean APACHE II score was 20.3 (SD 8.2). The subdistribution hazard ratio for time to successful extubation was 1.09 (95 percent CI 0.96 to 1.25, P = 0.20) for dexmedetomidine versus propofol, and 1.05 (95 percent CI 0.95 to 1.17, P = 0.34) for clonidine versus propofol. Median time from randomisation to extubation was 136 hours (95 percent CI 117 to 150) for dexmedetomidine, 146 hours (95 percent CI 124 to 168) for clonidine, and 162 hours (95 percent CI 136 to 170) for propofol.
The numerical direction of the point estimates favored the alpha-2 agonists. The confidence intervals crossed unity. Statistical significance was not met. ICU mortality at discharge was 21 percent for dexmedetomidine, 22 percent for clonidine, and 22 percent for propofol. At 90 days, mortality was 27 percent, 29 percent, and 29 percent respectively. At 180 days, 29 percent, 30 percent, and 30 percent.
The companion cost-effectiveness analysis (Morris and colleagues, JAMA Network Open, 2025) concluded that alpha-2 agonist sedation was unlikely to be cost-effective compared to propofol under the trial’s conditions.
The editorial that accompanied A2B in JAMA was titled to capture the moment exactly: the search for the single best sedative. The implication, written between the lines of any honest reading, is that the search itself may be the wrong project.
PADIS 2025: The focused update
The 2025 PADIS focused update (Lewis, Balas, Stollings, and colleagues, Crit Care Med, March 2025) was a methodologically rigorous re-examination of the 2018 PADIS guideline in light of new evidence. The task force pulled 29 RCTs comparing propofol and dexmedetomidine, against the three RCTs available in 2018.
The conditional recommendation: in mechanically ventilated adult ICU patients where light sedation and/or reduction in delirium are the highest priorities, use dexmedetomidine over propofol. Certainty of evidence: moderate. Strength: conditional.
This is not a strong recommendation. The guideline authors were explicit that this is a context-dependent suggestion. The bedside translation, however, is often less careful than the guideline text. “PADIS says use dex” became the institutional shorthand at many centers.
The prior literature
The A2B and PADIS conclusions both sit inside a literature that has been internally inconsistent for fifteen years.
SEDCOM (Riker and colleagues, JAMA 2009): dexmedetomidine reduced delirium prevalence compared with midazolam. MIDEX and PRODEX (Jakob and colleagues, JAMA 2012): dexmedetomidine was non-inferior to midazolam and propofol for sedation depth. DESIRE (Kawazoe and colleagues, JAMA 2017): in septic patients on mechanical ventilation, dexmedetomidine did not improve mortality or ventilator-free days at 28 days compared with usual care. SPICE-III (Shehabi and colleagues, NEJM 2019): early dexmedetomidine did not reduce 90-day mortality compared with usual care across 4,000 patients. The SPICE-III heterogeneity-of-treatment-effect analysis (Shehabi and colleagues, Intensive Care Med 2021): patients older than 65 had a 97.7 percent posterior probability of reduced mortality on dexmedetomidine. MENDS-II (Hughes and colleagues, NEJM 2021): in 432 septic ventilated adults, no difference in days alive without delirium or coma between dexmedetomidine and propofol.
A reasonable reader of this literature could conclude many things. One conclusion is that dexmedetomidine is modestly better in older patients. Another is that the agent matters less than the depth of sedation. Another is that the trial designs have varied enough that we have been comparing different questions. All three are defensible.
What is not defensible is the position that the field has settled on a “right answer” at the bedside. It has not.
Listen to the following podcast:
What Stood Out
Three things stood out to me from the A2B report.
First, the magnitude of the propofol re-rescue. Supplemental propofol was permitted in all three arms when the target sedation level could not be achieved with the primary agent. In the alpha-2 agonist arms, propofol re-rescue was common. This is not new (SPICE-III and DESIRE had the same pattern), but A2B confirms it at scale in a 2025 pragmatic environment. The implication: a “dexmedetomidine-based” sedation strategy in real-world ICUs is often a propofol-supplemented dex strategy. The pure-agent comparison is somewhat theoretical.
Second, the agitation signal. Both alpha-2 arms had numerically more agitation than the propofol arm in early sedation. This matters because agitation is precisely what every advocate of dexmedetomidine claims it reduces. The A2B authors were honest about this. The field is going to have to be honest about it too.
Third, the cost-effectiveness verdict. The Morris paper concluded that alpha-2 agonist sedation was unlikely to be cost-effective at conventional willingness-to-pay thresholds. In a year when every health system in the United States and Europe is under cost pressure, “we cannot prove a clinical benefit and the drug is much more expensive” is a hard argument to override at the formulary committee.
A “dexmedetomidine-based” sedation strategy in real-world ICUs is often a propofol-supplemented dex strategy. The pure-agent comparison is somewhat theoretical.
Interpretation: The Agent Is Not the Question
Here is my position. I have held it for five years. The 2025 evidence reinforces it.
The agent is not the question. The strategy is the question.
What the bedside actually wants to know is whether the patient in front of us is going to come off the ventilator faster, develop less delirium, mobilize sooner, and avoid the long-term cognitive consequences of ICU sedation. None of those outcomes are governed primarily by whether the drip in the IV pole says dexmedetomidine or propofol. They are governed by the depth of sedation, the rigor of daily reassessment, the discipline of the spontaneous breathing trial, the implementation of the ABCDEF bundle, and the team’s willingness to push toward RASS 0 to -1 rather than RASS -3 to -4 by default.
A patient kept lightly sedated on propofol will do better than a patient kept deeply sedated on dexmedetomidine. We have evidence from the original SPICE I observational work that deep sedation in the first 48 hours is independently associated with higher mortality, longer ventilation, and more delirium. That signal does not care about the chemical structure of the sedative.
This is why A2B and PADIS can both be right at the same time. PADIS is right that in the specific clinical scenario where light sedation and reduced delirium are the highest priorities, the meta-analytic signal favors dexmedetomidine. A2B is right that in the broader pragmatic ICU population, agent choice does not change the time-to-extubation needle. The reason both can be true is that the meta-analytic signal lives inside a specific subgroup (older patients targeted to light sedation, willing to tolerate bradycardia) while the pragmatic population is broader and more heterogeneous.
The bedside translation is not “use dex” or “use propofol.” It is this:
Pick the agent that fits the patient. Pick the depth that fits the goal. Reassess every shift. The depth conversation is more important than the agent conversation.
⸻
Bedside and Workplace Takeaways
1. Intensivists writing sedation orders. Stop thinking of the order as “start dexmedetomidine” or “start propofol.” Think of it as “target RASS 0 to -1 with the agent that best fits this patient’s hemodynamics and sepsis status.” Specify the target. Specify the reassessment cadence. If the team is targeting RASS -3 by default, no agent will save you.
2. Respiratory therapists running SBTs. A patient on dexmedetomidine may pass an SBT with hemodynamic patterns that look very different from a patient on propofol. Dex preserves respiratory drive better but produces more bradycardia. Build your SBT protocols to account for both. Document the pre-SBT RASS. The depth at which the SBT was run is more clinically useful than the agent.
3. ICU nurses titrating sedation. Watch for the bradycardia signal specifically. A2B and SPICE-III both showed it. Your unit’s threshold for calling a bradycardia event should be lower on dexmedetomidine, especially in patients with conduction system disease or beta blocker use. Document RASS every two to four hours. The titration cadence is the lever, not the agent.
4. Advanced practice providers managing the trajectory. You are often the one writing the transition order from propofol to dexmedetomidine for “delirium prevention” or “weaning preparation.” A2B does not support this transition as a routine maneuver. Reserve the agent change for specific clinical reasons (need to preserve respiratory drive during a difficult wean, intolerance of propofol due to triglycerides or propofol-related infusion physiology, specific delirium prevention indication in an older patient). Otherwise, optimize the strategy you already have.
5. Critical care pharmacists stewarding the formulary. The Morris cost-effectiveness data gives you an evidence-based lever for stewardship. Dexmedetomidine still has a role. It is no longer the default agent. Build order-set guardrails that ask the prescriber to specify the clinical indication for dex (delirium prevention in older patients, need to preserve respiratory drive, intolerance of propofol). The cost data backs you up.
6. Perfusionists and CV-ICU teams. The cardiac surgical literature on dexmedetomidine is more favorable than the general ICU literature. The post-bypass population is the one place where the meta-analytic signal for reduced delirium and reduced post-operative atrial fibrillation has held up most consistently. Your CV-ICU practice can defensibly diverge from your MICU practice on this. Do not assume the A2B pragmatic signal applies in the same way to the post-cardiotomy patient population.
⸻
Teaching Pearl
The single concept worth teaching from this controversy:
When a high-quality guideline and a high-quality pragmatic RCT disagree in the same year, they are usually answering different questions. The guideline pools across populations and outcomes to find a signal. The pragmatic trial preserves the heterogeneity of real-world practice and asks whether the signal survives. Both are useful. Neither is the final word.
The discipline at the bedside is to ask which question matches the patient in front of you. If the patient is an older mechanically ventilated adult where delirium prevention is the priority, the guideline signal applies. If the patient is a younger, hemodynamically labile, heterogeneously diagnosed ventilated patient where the question is “what do I start this morning,” the pragmatic data applies. The trick is being honest about which patient is in the bed.
This is what evidence-based practice actually looks like. It is not picking a side. It is matching the question to the patient.
A patient kept lightly sedated on propofol will do better than a patient kept deeply sedated on dexmedetomidine. The depth conversation is more important than the agent conversation.
What We Should Not Over-Assume
A few things the field is at risk of over-extrapolating from A2B and PADIS 2025.
Do not over-assume that A2B closes the door on dexmedetomidine. It does not. The trial population was broad, the comparisons were pragmatic, and the alpha-2 agonist arms allowed propofol re-rescue. The trial says dex is not a universal upgrade. It does not say dex has no role.
Do not over-assume that PADIS 2025 is a strong endorsement. The recommendation was conditional, with moderate certainty of evidence. The guideline authors were careful. The bedside often is not. “PADIS recommends dex” is a stronger claim than the document actually makes.
Do not over-assume that the older-patient subgroup signal from SPICE-III HTE is a license to use dex in every patient over 65. The Bayesian probability was high, but the absolute mortality difference was modest, and the confidence interval included the null at one boundary. Reasonable people can read the SPICE-III HTE analysis as suggestive rather than definitive.
Do not over-assume that cost-effectiveness is the same as cost. Dexmedetomidine has become substantially cheaper in the United States since the generic launch. The cost-effectiveness threshold conversation in 2026 is different from the 2018 conversation. Run your own institutional analysis.

Limitations
A2B is a UK-centric trial. UK sedation practice has historically been lighter than US practice, and the propofol comparator in A2B may have been delivered in a way that already approximated best practice. The generalizability to a US ICU still anchored at deeper sedation may favor dexmedetomidine more than A2B suggests, because the US “usual care” comparator is not the same as the UK “usual care” comparator.
A2B was open-label. Sedation trials are difficult to blind, and the open-label design carries an unavoidable risk of performance bias.
The trial population required at least 48 hours of expected mechanical ventilation. Patients ventilated for shorter durations are not represented. The high-volume short-stay ICU population (post-operative recoveries, brief respiratory failure) is outside the trial’s inference space.
PADIS 2025 was a focused update, not a full guideline reconstruction. Several relevant clinical questions (depth of sedation, ABCDEF bundle implementation, sedation in specific subpopulations) were either out of scope or addressed in the 2018 guideline and not revisited.
The trials in the meta-analytic base for PADIS 2025 were heterogeneous in sedation depth, comparator drugs, and outcome measurement. The 29 RCTs are not 29 versions of the same study. The pooled signal hides as much as it reveals.
Bottom Line
The 2025 PADIS focused update and the 2025 A2B trial point in different directions because they answer different questions. The guideline says dex is modestly better in the specific scenario of light-sedation-targeted, delirium-prevention-prioritized care. The trial says it does not improve the broader pragmatic outcome of time to extubation. Both are right.
The agent is not the lever. The depth is the lever. The reassessment cadence is the lever. The discipline of the ABCDEF bundle is the lever. Pick the agent that fits the patient and stop arguing about which agent fits everyone.
Your sedation rounds tomorrow should ask the same three questions they should have been asking in 2018: What is the target RASS, who is responsible for reassessing it every shift, and what is the daily plan for lightening sedation toward an SBT?
Get those right and the agent argument becomes a footnote.
References
Walsh TS, Parker RA, Aitken LM, et al. Dexmedetomidine- or clonidine-based sedation compared with propofol in critically ill patients: the A2B randomized clinical trial. JAMA. 2025;334(1):32-45. doi:10.1001/jama.2025.7200
Lewis K, Balas MC, Stollings JL, et al. A focused update to the clinical practice guidelines for the prevention and management of pain, anxiety, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2025;53(3):e711-e727.
Qian ET, Rice TW. The search for the single best sedative. JAMA. 2025;334(1):26-28. doi:10.1001/jama.2025.7359
Morris S, Lone NI, McKenzie CA, et al. Cost-effectiveness of α2 agonists for intravenous sedation in patients with critical illness. JAMA Netw Open. 2025;8(5):e2517533. doi:10.1001/jamanetworkopen.2025.17533
Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825-e873.
Shehabi Y, Howe BD, Bellomo R, et al. Early sedation with dexmedetomidine in critically ill patients. N Engl J Med. 2019;380(26):2506-2517. doi:10.1056/NEJMoa1904710
Shehabi Y, Serpa Neto A, Howe BD, et al. Early sedation with dexmedetomidine in ventilated critically ill patients and heterogeneity of treatment effect in the SPICE III randomised controlled trial. Intensive Care Med. 2021;47(4):455-466. doi:10.1007/s00134-021-06356-8
Hughes CG, Mailloux PT, Devlin JW, et al. Dexmedetomidine or propofol for sedation in mechanically ventilated adults with sepsis. N Engl J Med. 2021;384(15):1424-1436. doi:10.1056/NEJMoa2024922
Kawazoe Y, Miyamoto K, Morimoto T, et al. Effect of dexmedetomidine on mortality and ventilator-free days in patients requiring mechanical ventilation with sepsis: a randomized clinical trial. JAMA. 2017;317(13):1321-1328. doi:10.1001/jama.2017.2088
Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301(5):489-499. doi:10.1001/jama.2009.56
Jakob SM, Ruokonen E, Grounds RM, et al. Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012;307(11):1151-1160. doi:10.1001/jama.2012.304
Strøm T, Martinussen T, Toft P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet. 2010;375(9713):475-480. doi:10.1016/S0140-6736(09)62072-9
Olsen HT, Nedergaard HK, Strøm T, et al. Nonsedation or light sedation in critically ill, mechanically ventilated patients. N Engl J Med. 2020;382(12):1103-1111. doi:10.1056/NEJMoa1906759
Marra A, Ely EW, Pandharipande PP, Patel MB. The ABCDEF bundle in critical care. Crit Care Clin. 2017;33(2):225-243. doi:10.1016/j.ccc.2016.12.005
Pun BT, Balas MC, Barnes-Daly MA, et al. Caring for critically ill patients with the ABCDEF bundle: results of the ICU liberation collaborative in over 15,000 adults. Crit Care Med. 2019;47(1):3-14. doi:10.1097/CCM.0000000000003482
Clinical Disclaimer
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.
Javier Amador-Castaneda, BHS, RRT, FCCM | Founder & CEO, ICCN