

When Do You Call It After Cardiac Arrest? A Fresh 2026 Framework Says the Honest Answer Is Later Than Your Unit Is Calling It Now.

A March 2026 Frontiers in Medicine framework by Kortli and Nasa pulls together what fifteen years of post-cardiac arrest research has been telling us. Monomodal prognostication is dangerous. The 72-hour clock is too fast for many patients. The self-fulfilling prophecy is the field’s largest unmeasured bias. Here is the ICCN read.
In a 24-hour ICU, the most consequential decision the team makes on a post-cardiac arrest patient is not what vasopressor to use, what oxygen target to set, or what temperature to target. The most consequential decision is when to declare that the brain will not recover.
The decision is consequential because it is irreversible. Once life-sustaining therapy is withdrawn on the basis of a prognostication call, the prophecy fulfills itself. The patient dies. The outcome data the field uses to build its prognostic tools is built on patients in whom prognostication preceded withdrawal. The field has been measuring its own predictions.
This is the self-fulfilling prophecy problem. It is the largest unmeasured bias in the post-cardiac arrest literature. It is the reason a March 2026 Frontiers in Medicine framework by Kortli and Nasa has landed with weight in the post-cardiac arrest community: it pulls together fifteen years of evidence into a clean, multimodal, delayed-prognostication approach that takes the self-fulfilling prophecy seriously.
Today’s Saturday piece is the ICCN read on what the 2026 framework gets right, what the bedside still has to confront, and how every ICU should re-examine its prognostication discipline this quarter.
ICCN Update
The new ICCN website is live at iccn.io. Every article published in the past two weeks is now archived in one place, and our new Research section pulls recent published data from 26 major critical care and medical journals into a single curated feed for subscribers. Bookmark iccn.io.
Why This Matters
Out-of-hospital cardiac arrest has approximately a 10 percent survival to hospital discharge globally. In-hospital cardiac arrest survival is somewhat higher, but the comatose post-arrest survivor remains one of the highest-acuity, longest-staying, most resource-intensive populations any ICU manages.
The cost of getting prognostication wrong cuts both ways. If the team declares poor prognosis too early and withdraws care on a patient who would have recovered, the loss is irrecoverable. If the team continues aggressive care indefinitely on a patient who will not recover, the patient suffers, the family suffers, and the ICU absorbs resources that other patients need.
The field’s response to this tension over the past fifteen years has been to develop increasingly sophisticated multimodal prognostication. The 2014 ERC-ESICM advisory. The 2021 ERC-ESICM post-cardiac arrest guideline. The TTM2 trial in 2021. The BOX trial in 2022. The Neurocritical Care Society guidelines in 2023. The 2024 AHA scientific statement. And now the 2026 Kortli-Nasa framework.
If you are an intensivist running the post-arrest pathway, an RT managing the ventilator through the prognostication window, an ICU nurse performing the neurological exam and supporting the family, an APP coordinating the workup, a pharmacist managing the sedation washout, or a perfusionist supporting an ECPR survivor, this story lands directly on your practice.
The 2026 framework matters because it takes the position the field has been moving toward for a decade and writes it down clearly: prognostication is multimodal, delayed, and integrated. Anything less is below standard of care in 2026.
The Study and the Evidence in Context
The 2026 framework: what Kortli and Nasa actually propose
The Kortli-Nasa framework is a narrative review and clinical framework, not a randomized trial. It is the kind of paper the field needed. It synthesizes the multimodal post-cardiac arrest literature, organizes it around brain recovery rather than only around mortality, and offers a clinical structure for the bedside.
The framework has three core elements.
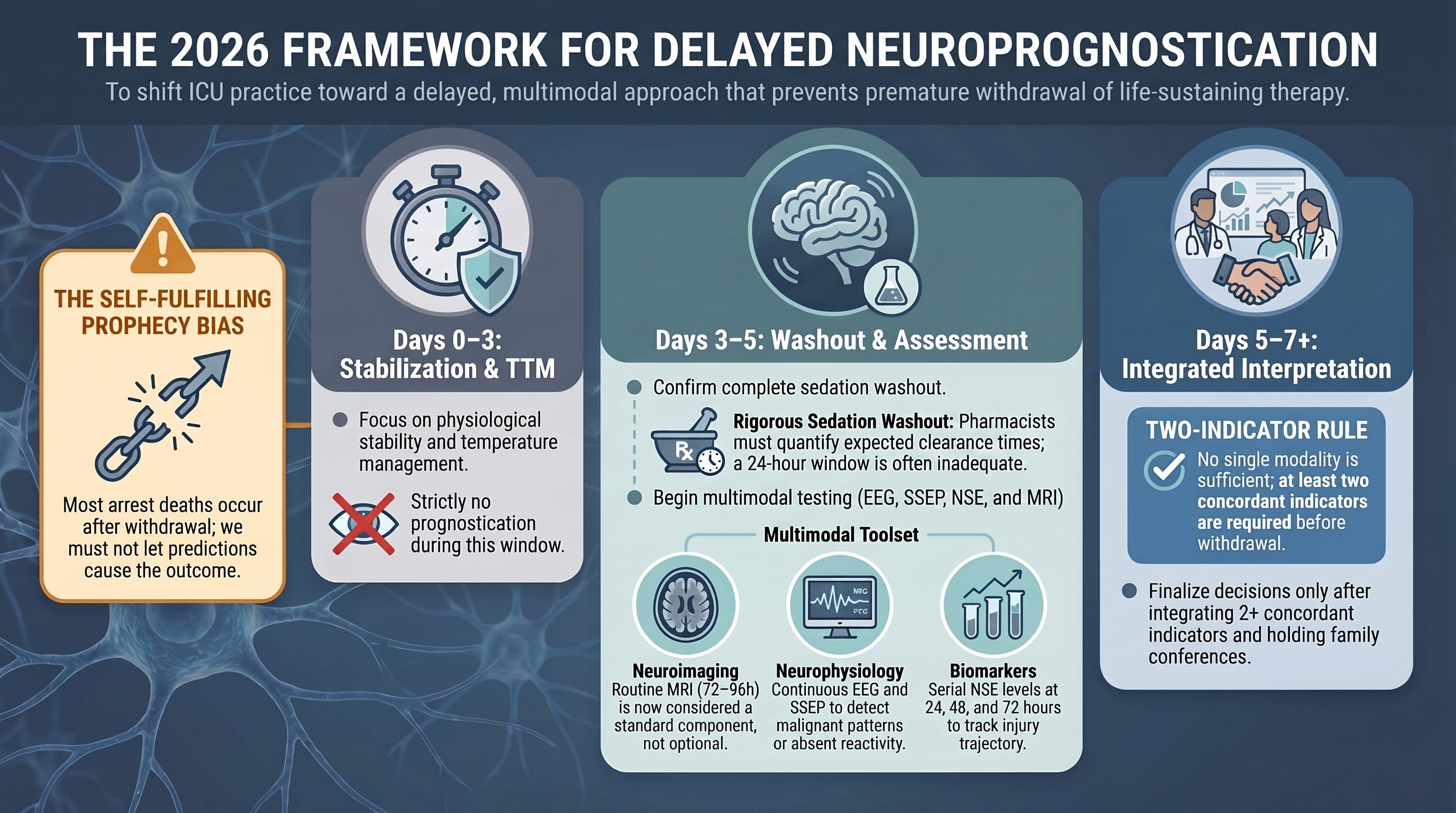
1. Brain recovery as the primary outcome of interest. The traditional post-cardiac arrest endpoint has been mortality or the Cerebral Performance Category (CPC) score. The Kortli-Nasa framing emphasizes the trajectory of neurological recovery itself, including delayed awakening, late motor improvement, and cognitive recovery that may extend weeks to months past ICU discharge. This reframing has clinical implications: it argues against premature closure on prognostication and for active brain-recovery interventions during the acute period.
2. Multimodal prognostication as the only defensible approach. The framework formalizes what the 2021 ERC-ESICM guideline already recommended. No single modality (clinical exam, EEG, SSEP, NSE, neuroimaging, pupillometry) is sufficient to declare poor prognosis. Each has false-positive rates that, applied universally, would cause unacceptable rates of withdrawal in patients who would have recovered. The framework reiterates that two or more concordant indicators are required before withdrawal of life-sustaining therapy can be discussed.
3. Timing discipline. The framework explicitly endorses delayed prognostication. The conventional 72-hour mark is the earliest reasonable window, not the recommended one. In patients on TTM or with significant sedation exposure, the framework supports extending prognostication to day 5, day 7, or beyond, with sedation washout treated as a precondition rather than a footnote. The 2024 ICECAP trial of extended cooling and the 2026 literature on delayed neurological recovery both support this discipline.
The trial evidence the framework sits on
TTM2 (Dankiewicz et al, NEJM 2021). 1,900 patients randomized to targeted temperature 33 degrees Celsius versus normothermia with fever control. No mortality difference at six months. Reframed the temperature question from “which target” to “fever prevention” as the active ingredient. The 2024 AHA scientific statement and 2025 ILCOR consensus integrated this finding.
BOX (Schmidt et al, NEJM 2022). Factorial trial of oxygen target (8-10 vs 13-14 kPa) and MAP target (63 vs 77 mmHg) in 789 OHCA patients. No significant differences in primary outcomes. Practice took the finding as permission to target a wider physiologic range.
ICECAP (Hsu et al, NEJM 2024). Trial of 12-hour versus longer-duration (24-48 hour) targeted temperature management. Did not show benefit of longer cooling. Reinforced the move toward shorter, fever-controlled, individualized temperature management.
Multimodal prognostication evidence base. The 2020 Sandroni systematic review in Intensive Care Medicine confirmed that no single tool has acceptable false-positive rates. The 2023 Neurocritical Care Society guidelines codified multimodal use. The 2024 AHA statement reinforced delayed timing.
The self-fulfilling prophecy literature. Mulder and colleagues (Crit Care Med 2014) and follow-up work have documented that the majority of post-arrest deaths in the ICU occur after withdrawal of life-sustaining therapy. The implication is that the field’s prognostic models are trained on a population in which the outcome was, in part, chosen by the clinical team. Untangling true biological prognosis from clinical-decision-driven outcome remains methodologically difficult.
Why the framework lands now
The 2026 publication date is not incidental. The field has accumulated enough trial and observational evidence over the past five years to make the framework’s recommendations defensible. The bedside has not always implemented them. The Kortli-Nasa synthesis is doing what good framework papers do: pulling the existing evidence into a structure clinicians can apply on Monday morning.
What Stood Out
Three elements of the 2026 framework stood out.
1. The explicit endorsement of delayed prognostication. The framework does not hedge. It says that 72 hours is the earliest reasonable timepoint, that sedation washout must be confirmed before prognostication, and that day 5 to 7 is often more appropriate. This is a meaningful tightening of the language used in earlier guidelines.
2. The integration of neuroimaging as a routine component. The framework treats neuroimaging (MRI especially) as a standard part of multimodal prognostication rather than an optional add-on. Many ICUs still do not routinely MRI post-arrest patients. The framework argues this should change.
3. The honest treatment of the self-fulfilling prophecy. The framework acknowledges directly that the field’s outcome data is shaped by withdrawal decisions, and that this introduces a circular epistemology into the prognostic literature. Few framework papers in this space have been this transparent. The acknowledgment matters because it justifies the delayed-prognostication discipline on epistemic as well as clinical grounds.
The field has been measuring its own predictions. The 2026 framework is the first to say so this plainly. The bedside discipline now has to catch up.
Interpretation: The Framework Is the Field’s Best 2026 Synthesis. Implementation Will Be the Hard Part.
Here is the ICCN position.
The Kortli-Nasa framework is the cleanest 2026 synthesis of where the post-cardiac arrest community has been moving for a decade. None of its individual recommendations are new. The integration is what is new, and the integration is what the bedside needs.
The implementation challenge is not evidence-based. It is operational. Three structural barriers persist:
1. Sedation washout discipline. In a patient who received propofol, midazolam, or fentanyl boluses for the duration of TTM, sedation washout takes longer than most teams assume. A 24-hour washout is often inadequate. The bedside still tends to evaluate the neurological exam before pharmacologic confounding has cleared. The framework’s call for delayed prognostication implicitly demands stricter sedation washout discipline.
2. Multimodal availability. Not every ICU has 24/7 access to EEG, SSEP, NSE, and MRI. The framework’s multimodality assumes resource availability that not every unit has. The bedside translation in resource-limited settings has to be: do what you can with what you have, document it, and resist single-modality prognostication when the alternative is no prognostication at all.
3. Family communication and the moral burden of waiting. Delayed prognostication imposes a moral burden on the family. Five to seven days of uncertainty is hard. Some families want a faster answer. The framework’s discipline holds only if the team is willing to communicate honestly that the team does not yet know, that the team will know, and that the timeline is informed by the patient’s safety rather than by clinician discomfort with uncertainty.
The Saturday position: in 2026, no ICU should be making withdrawal decisions on a post-cardiac arrest patient before 72 hours of fully washed-out, multimodal assessment, except in the small subset of patients with overwhelming, concordant indicators of devastating brain injury (loss of multiple brainstem reflexes, malignant EEG with no reactivity, absent N20s, devastating MRI, and a sustained clinical exam consistent with brain death).
Everyone else gets time. The patients we are most afraid of misclassifying are exactly the patients who deserve the discipline.
Bedside and Workplace Takeaways
1. Intensivists running the post-arrest pathway. Build a protocol that explicitly defines the prognostication window. Day 0 to 3 is stabilization. Day 3 to 5 is multimodal assessment after sedation washout. Day 5 to 7 is integrated interpretation and family conference. No withdrawal discussions before that timeline except in the rare overwhelming case. Document the rationale in the chart.
2. Respiratory therapists supporting ventilation through the prognostication window. Stability of oxygenation, normocapnia, and absence of asynchrony all matter to the validity of the neurological exam. Hypercapnia can cause apparent obtundation. Hyperoxia may be deleterious post-arrest. Maintain target PaO2 in the normal range. Avoid permissive hypercapnia during the prognostication window unless clinically required.
3. ICU nurses performing the neurological exam and supporting the family. Your serial exams are the foundation of the prognostication picture. Document GCS components separately. Document brainstem reflexes individually. Document motor response by limb. The trajectory matters as much as the snapshot. On the family communication side, the line that helps most is honesty about timing: we will know in five to seven days, we do not know now, we will tell you what we find as we find it.
4. Advanced practice providers coordinating the workup. Build a standardized order set that triggers EEG, SSEP, NSE at 24, 48, and 72 hours, MRI at 72 to 96 hours (with the team’s neuroimaging service), and pupillometry where available. The standardization reduces the chance that any single modality drives a premature conclusion.
5. Critical care pharmacists managing sedation washout. This is where pharmacy has direct prognostic impact. Build a sedation washout pathway. Quantify expected washout time based on the agents used (fentanyl with renal failure may take days; propofol clears faster; benzodiazepines accumulate in renal/hepatic dysfunction). Communicate to the team when the exam can be considered drug-free.
6. Perfusionists and ECPR coordinators. ECPR survivors are a distinct prognostic population. The ARREST trial and follow-up literature suggest some ECPR patients have meaningful neurological recovery even after prolonged low-flow times. Your team’s involvement in the prognostic discussion should reflect the unique recovery trajectory of this population.
Listen to the following podcast:
Teaching Pearl
The single concept worth teaching from this framework:
The field’s prognostic models are trained on a dataset shaped by its own withdrawal decisions. This is the self-fulfilling prophecy problem. The bedside response is not to abandon prognostication. The bedside response is to delay it, multimodalize it, integrate it, and treat the question of when to call it with the same epistemic discipline the question of how to call it has received.
Teach this in resuscitation grand rounds. Teach it in neurocritical care fellowship. Teach it in nursing competency review. The next generation of clinicians should inherit the framework as the default approach, not as the aspirational ideal.
Five to seven days of uncertainty is hard. It is also the discipline the evidence demands. The patients we are most afraid of misclassifying are exactly the patients who deserve that time.
What We Should Not Over-Assume
1. Do not over-assume that multimodal means “more tests is always better.” The framework supports multimodality because no single tool is reliable, not because more data is universally better. In a patient with overwhelming clinical findings concordant across modalities, additional testing may not change the management. The discipline is about integration and timing, not about volume of investigations.
2. Do not over-assume that delayed prognostication means indefinite continuation. The framework supports delayed assessment because early assessment is unreliable. It does not support continuation of aggressive care in the face of concordant multimodal evidence of devastating brain injury. The right answer is the right timing combined with the right rigor.
3. Do not over-assume that the framework applies identically to every post-arrest population. Out-of-hospital arrest, in-hospital arrest, witnessed versus unwitnessed, shockable versus non-shockable, ECPR versus conventional resuscitation — these populations have different prognostic baselines. The multimodal architecture applies. The interpretation of individual modalities may shift by population.
4. Do not over-assume that the self-fulfilling prophecy invalidates the prognostic literature. It complicates it. The literature still informs clinical decision-making. The bedside lesson is to hold prognostic confidence with appropriate epistemic humility, especially in patients with discordant findings.
5. Do not over-assume that family preferences resolve the uncertainty. Some families want fast answers. Some want continued aggressive care. The framework’s discipline holds regardless of family preference, because the question being answered is biological prognosis, not value preference. Value preferences belong in the family conference after the biological prognosis is established.
Limitations
The Kortli-Nasa paper is a narrative review and clinical framework. It is not a systematic review and not a primary trial. Narrative reviews have inherent selection bias.
The framework’s recommendations on multimodal prognostication and delayed timing are well-supported by the existing literature, but the absolute false-positive rates for combined modalities have not been definitively established in adequately powered, contemporary, prospectively-collected cohorts. The literature relies heavily on retrospective and observational data.
The self-fulfilling prophecy critique applies to the framework’s own evidence base. We do not have a clean dataset of post-arrest patients in whom withdrawal of life-sustaining therapy did not occur, against which we could calibrate the true biological prognostic value of any modality.
The framework was published in Frontiers in Medicine (Lausanne). Some readers regard the Frontiers journals as varying in editorial rigor across articles. The peer review process is transparent and the article is open access. Reasonable readers can have differing views on the editorial weight of this specific outlet. The framework’s conclusions align closely with the 2021 ERC-ESICM guidelines, the 2023 Neurocritical Care Society guidelines, and the 2024 AHA scientific statement, which supports the case that the framework reflects current consensus rather than idiosyncratic interpretation.
The framework does not address the question of how the prognostic discipline interacts with organ donation pathways, which are increasingly relevant in some post-arrest populations.
Bottom Line
When do you call it after cardiac arrest? The 2026 Kortli-Nasa framework gives the bedside the clearest synthesis of the past fifteen years of evidence. The answer it endorses is: not before 72 hours of fully washed-out, multimodal assessment. In many patients, the right timing is day 5 to 7. The discipline is multimodal, integrated, and explicitly aware of the self-fulfilling prophecy.
If your unit is making withdrawal decisions on post-cardiac arrest patients before that window, on the basis of single-modality findings, or before sedation washout, your prognostication discipline is out of step with the 2026 standard of care. The implementation gap is operational, not evidentiary. Build the protocol. Standardize the order set. Steward the sedation washout. Communicate honestly with families about the timeline. The bedside that does this in 2026 will produce better outcomes than the bedside that does not.
References
Kortli S, Nasa P. The neurological phoenix: multimodal strategies for brain recovery and prognostication in post-cardiac arrest syndrome — a 2025 clinical framework. Front Med (Lausanne). 2026;13:1775538. doi:10.3389/fmed.2026.1775538
Dankiewicz J, Cronberg T, Lilja G, et al; TTM2 Trial Investigators. Hypothermia versus normothermia after out-of-hospital cardiac arrest. N Engl J Med. 2021;384(24):2283-2294. doi:10.1056/NEJMoa2100591
Schmidt H, Kjaergaard J, Hassager C, et al. Oxygen targets in comatose survivors of cardiac arrest. N Engl J Med. 2022;387(16):1467-1476. doi:10.1056/NEJMoa2208686
Kjaergaard J, Møller JE, Schmidt H, et al. Blood-pressure targets in comatose survivors of cardiac arrest. N Engl J Med. 2022;387(16):1456-1466. doi:10.1056/NEJMoa2208687
Nolan JP, Sandroni C, Böttiger BW, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021;47(4):369-421. doi:10.1007/s00134-021-06368-4
Sandroni C, D’Arrigo S, Cacciola S, et al. Prediction of poor neurological outcome in comatose survivors of cardiac arrest: a systematic review. Intensive Care Med. 2020;46(10):1803-1851. doi:10.1007/s00134-020-06198-w
Rajajee V, Muehlschlegel S, Wartenberg KE, et al. Guidelines for neuroprognostication in comatose adult survivors of cardiac arrest. Neurocrit Care. 2023;38(3):533-563. doi:10.1007/s12028-023-01688-3
Geocadin RG, Callaway CW, Fink EL, et al. Standards for studies of neurological prognostication in comatose survivors of cardiac arrest: a scientific statement from the American Heart Association. Circulation. 2019;140(9):e517-e542. doi:10.1161/CIR.0000000000000702
Hofmeijer J, Tjepkema-Cloostermans MC, van Putten MJAM. Burst-suppression with identical bursts: a distinct EEG pattern with poor outcome in postanoxic coma. Clin Neurophysiol. 2014;125(5):947-954. doi:10.1016/j.clinph.2013.10.017
Mulder M, Gibbs HG, Smith SW, et al. Awakening and withdrawal of life-sustaining treatment in cardiac arrest survivors treated with therapeutic hypothermia. Crit Care Med. 2014;42(12):2493-2499. doi:10.1097/CCM.0000000000000540
Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396(10265):1807-1816. doi:10.1016/S0140-6736(20)32338-2
Sandroni C, Cariou A, Cavallaro F, et al. Prognostication in comatose survivors of cardiac arrest: an advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Resuscitation. 2014;85(12):1779-1789. doi:10.1016/j.resuscitation.2014.08.011
Lybeck A, Friberg H, Aneman A, et al. Prognostic significance of clinical seizures after cardiac arrest and target temperature management. Resuscitation. 2017;114:146-151. doi:10.1016/j.resuscitation.2017.01.017
Beekman R, Hirsch KG. Brain imaging after cardiac arrest. Curr Opin Crit Care. 2023;29(3):192-198. doi:10.1097/MCC.0000000000001037
Berg KM, Soar J, Andersen LW, et al; Adult Advanced Life Support Collaborators. Adult advanced life support: 2024 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2024;205:110414.
Eertmans W, Genbrugge C, Vander Laenen M, et al. The prognostic value of bispectral index and suppression ratio monitoring after out-of-hospital cardiac arrest: a prospective observational study. Ann Intensive Care. 2018;8(1):34. doi:10.1186/s13613-018-0380-z
Hsu CH, Couper K, Nix T, et al; ICECAP Investigators. Duration of cooling with 33°C after out-of-hospital cardiac arrest: the ICECAP randomized clinical trial. N Engl J Med. 2024.
Clinical Disclaimer
⚠️ Medical Disclaimer: The content published in ICCN is intended solely for educational and informational purposes for healthcare professionals. It does not constitute medical advice, clinical guidelines, or a standard of care, and should not be used as a substitute for the independent professional judgment of a licensed clinician. All clinical decisions must be individualized to the patient and made by qualified healthcare providers. ICCN assumes no liability for any clinical outcomes arising from the information presented herein.
© 2026 Interprofessional Critical Care Network (ICCN). All rights reserved. Unauthorized reproduction or redistribution of this content is prohibited. Subscribers may share excerpts with proper attribution to ICCN and the author.
Javier Amador-Castaneda, BHS, RRT, FCCM | Founder & CEO, ICCN